

Non-oliguric acute renal failure secondary to a potentially lethal dose of caffeine with acute intoxication: a case report
- PMID: 39695431
- PMCID: PMC11653949
- DOI: 10.1186/s12882-024-03905-3
Non-oliguric acute renal failure secondary to a potentially lethal dose of caffeine with acute intoxication: a case report
Abstract
Background: Recently, the incidence of caffeine intoxication has been on an upward trend, with severe outcomes. However, acute kidney injury (AKI) resulting from renal pathologies secondary to caffeine intoxication is rare, and the pathophysiological mechanisms underlying AKI are unclear.
Case presentation: A female patient in her 20s ingested an over-the-counter drug containing caffeine. The patient was diagnosed with secondary non oliguric AKI caused by acute intoxication due to ingestion of a lethal dose of caffeine. On day 19 of hospitalization, a renal biopsy was performed to determine the etiology of her prolonged renal dysfunction. Light microscopy revealed normal glomeruli, mild inflammatory cell infiltration, and acute tubular damage. Myoglobin staining was positive within the tubules, with scattered myoglobin columns. Electron microscopy revealed loss of glomerular epithelial foot processes and inflated tubular mitochondria. After undergoing hemodialysis and continuous hemodiafiltration, the patient's overall condition stabilized. After a consultation with a psychiatrist, on her 34th day of hospitalization, she was discharged home.
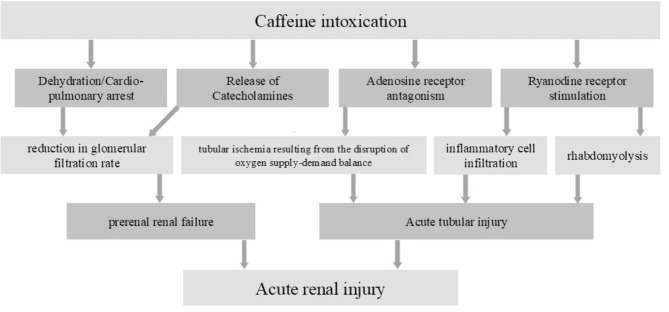
Conclusions: Caffeine antagonizes adenosine receptors, stimulates ryanodine receptors, and elevates catecholamines. The onset of AKI is hypothesized to result from a combination of these mechanisms, resulting in tubular ischemia and injury, as well as renal artery constriction. The development of AKI was thought to be caused by the following factors: (1) disruption of the tubular oxygen supply-demand ratio and consequent ischemia due to adenosine receptor antagonism by caffeine, (2) tubular damage due to rhabdomyolysis and consequent ryanodine receptor stimulation, and (3) increased catecholamine levels and consequent renal artery constriction.
Keywords: Acute caffeine intoxication; Acute kidney injury; Renal biopsy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval was not sought for the present study because a case report is a medical activity. Consent for publication: Written informed consent for publication of the clinical details was obtained from each of the patient and a copy of each consent form is available if requested by the Editor of the journal. Competing interests: The authors declare no competing interests.
Figures

References
-
- Hoffman RJ et al. Methylxanthines and selective β2-adrenergic agonists. In: Hoffmann RS, Howland MA, Lewin NA, eds. Goldfrank’s Toxicological Emergencies 10th ed. 2015; 909 – 20.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
