

Type 2 diabetes-related sarcopenia: role of nitric oxide
- PMID: 39695784
- PMCID: PMC11656607
- DOI: 10.1186/s12986-024-00883-z
Type 2 diabetes-related sarcopenia: role of nitric oxide
Abstract
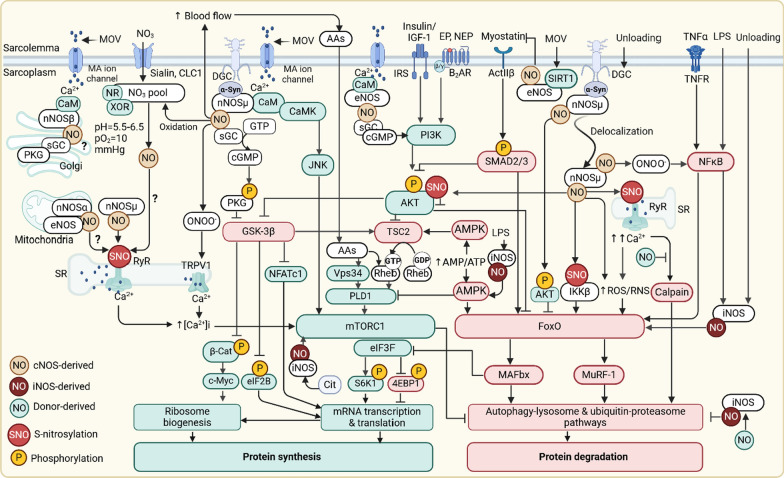
Sarcopenia, characterized by progressive and generalized loss of skeletal muscle (SkM) mass, strength, and physical performance, is a prevalent complication in type 2 diabetes (T2D). Nitric oxide (NO), a multifunctional gasotransmitter involved in whole-body glucose and insulin homeostasis, plays key roles in normal SkM physiology and function. Here, we highlight the role of NO in SkM mass maintenance and its potential contribution to the development of T2D-related sarcopenia. Physiologic NO level, primarily produced by sarcolemmal neuronal nitric oxide synthase (nNOSμ isoform), is involved in protein synthesis in muscle fibers and maintenance of SkM mass. The observed effect of nNOSμ on SkM mass is muscle-type specific and sex-dependent. Impaired NO homeostasis [due to a diminished nNOSμ-NO availability and excessive NO production through inducible NOS (iNOS) in response to atrophic stimuli, e.g., inflammatory cytokines] in SkM occurred during the development and progression of T2D, may cause sarcopenia. Theoretically, restoration of NO through nNOS overexpression, supplying NOS substrates (e.g., L-arginine and L-citrulline), phosphodiesterase (PDE) inhibition, and supplementation with NO donors (e.g., inorganic nitrate) may be potential therapeutic approaches to preserve SkM mass and prevents sarcopenia in T2D.
Keywords: L-arginine; Nitrate; Nitric oxide; Sarcopenia; Skeletal muscle mass; Type 2 diabetes.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
