

Are crystalloid-based fluid expansion strategies still relevant in the first hours of trauma induced hemorrhagic shock?
- PMID: 39695790
- PMCID: PMC11654417
- DOI: 10.1186/s13054-024-05185-7
Are crystalloid-based fluid expansion strategies still relevant in the first hours of trauma induced hemorrhagic shock?
Abstract
Background: Crystalloid-based fluid resuscitation has long been a cornerstone in the initial management of trauma-induced hemorrhagic shock. However, its benefit is increasingly questioned as it is suspected to increase bleeding and worsen coagulopathy. The emergence of alternative strategies like permissive hypotension and vasopressor use lead to a shift in early trauma care practices. Critical appraisal of current evidence is necessary to guide clinicians and outline research perspectives.
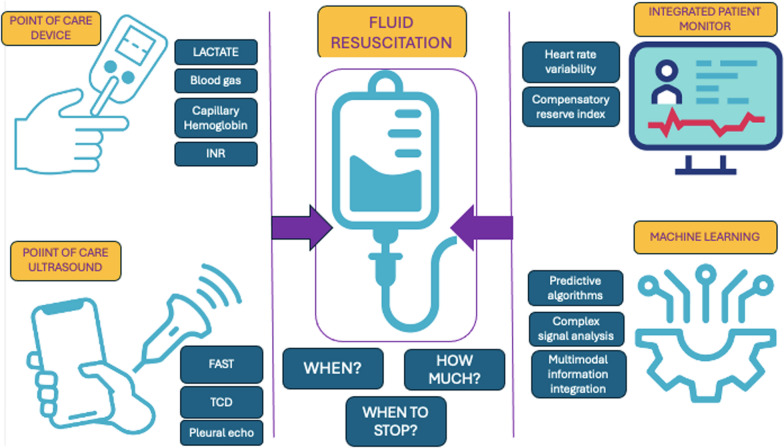
Main text: Current guidelines for managing trauma-induced hemorrhagic shock suggest titrating fluids and using vasopressors to achieve minimal blood pressure targets until hemorrhage is controlled. In case of traumatic brain injury with severe hemorrhage, blood pressure target increases. The scientific literature supporting these recommendations is limited, and several aspects remain the subject of ongoing scientific debate. The aim of this review is to evaluate the existing evidence on low-volume fluid resuscitation during the first hours of trauma management, with an emphasis on its integration with permissive hypotension, vasopressor use and cerebral perfusion pressure in traumatic brain injury. The review also highlights the limitations of current guidelines, particularly the lack of robust evidence supporting specific type of fluid, volumes and administration protocols tailored to specific trauma scenarios and populations. Emerging technologies such as point-of-care diagnostics, integrated monitoring systems, and machine learning hold promise for enhancing clinical decision-making in trauma care. These innovations could play a crucial role, ultimately helping clinicians address critical unanswered questions in trauma management and improve patient survival.
Conclusions: Crystalloid-based resuscitation remains relevant in early trauma care, but its application must be reassessed considering recent evidence and evolving practices. Further research is essential to refine fluid resuscitation guidelines, particularly in defining safe fluid volumes and the role of vasopressors. The integration of advanced monitoring technologies may offer new opportunities to optimize trauma care and improve outcomes.
Keywords: Advanced monitoring; Crystalloid fluids; Fluid resuscitation; Permissive hypotension; Trauma care; Trauma-induced hemorrhagic shock; Vasopressors.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
