

Seven versus 14 days of antimicrobial therapy for severe multidrug-resistant Gram-negative bacterial infections in intensive care unit patients (OPTIMISE): a randomised, open-label, non-inferiority clinical trial
- PMID: 39695798
- PMCID: PMC11653996
- DOI: 10.1186/s13054-024-05178-6
Seven versus 14 days of antimicrobial therapy for severe multidrug-resistant Gram-negative bacterial infections in intensive care unit patients (OPTIMISE): a randomised, open-label, non-inferiority clinical trial
Abstract
Background: Shorter courses of antimicrobial therapy have been shown to be non-inferior to longer durations for the management of several infections. However, data on critically ill patients with severe infections by multidrug-resistant Gram-negative bacteria (MDR-GNB) are scarce. In the duratiOn of theraPy in severe infecTIons by MultIdrug-reSistant gram-nEgative bacteria (OPTIMISE) trial, we assessed the non-inferiority of 7-day versus 14-day antimicrobial therapy for patients with intensive care unit (ICU)-acquired severe infections by MDR-GNB.
Methods: This was a randomised multicenter, open-label, parallel controlled, non-inferiority trial. Adult patients with severe infections by MDR-GNB initiated ≥ 48 h of ICU admission were eligible if they were hemodynamically stable and without fever > 48 h on the 7th day of appropriate antimicrobial therapy. Patients were 1:1 randomised to discontinue antimicrobial therapy on the 7th (± 1) day or to continue for a total of 14 (± 1) days. The primary outcome was clinical failure, defined as death or relapse of infection within 28 days of randomisation. An upper edge of the two-tailed 95% confidence interval (CI) of the delta between the clinical failure rate in the 7- and the 14-day lower than 10% in both intention-to-treat (ITT) and per protocol (PP) analyses was set as the non-inferiority criteria.
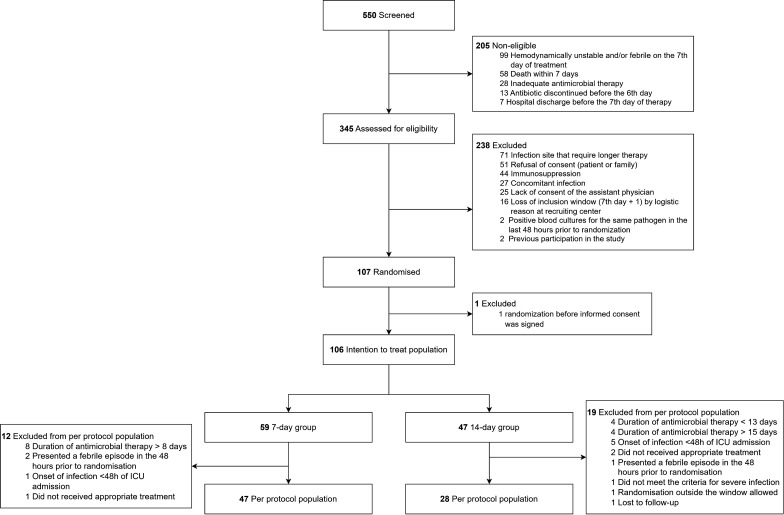
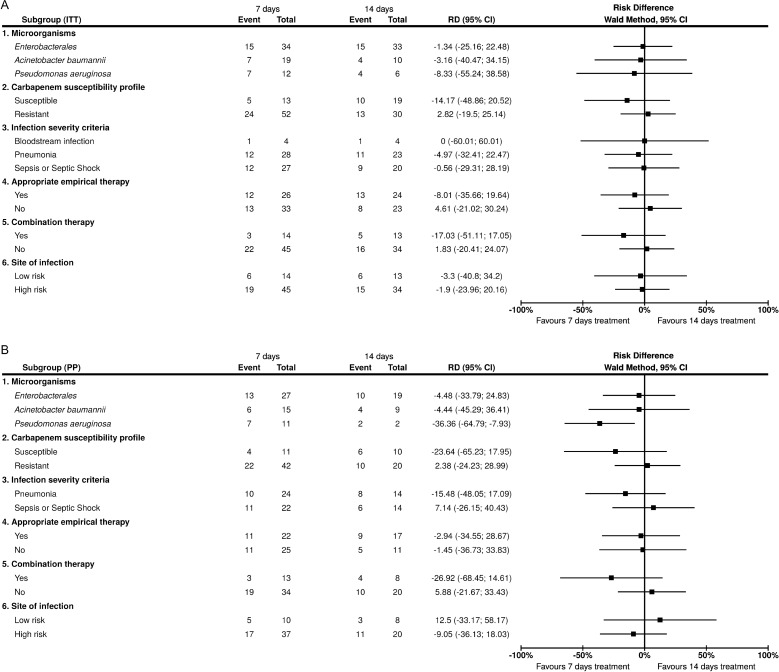
Results: A total of 106 patients composed the ITT population: 59 and 47 allocated to 7- and 14-day groups, respectively. The PP population included 75 patients: 47 and 28 in the 7- and 14-day groups, respectively. Clinical failure occurred in 42.4% and 44.7% of the ITT population in 7- and 14-day groups, respectively, (risk difference (RD) - 2.3, 95%CI - 21.3 to 16.7), and in 46.8% and 50.0% of the PP population in 7- and 14-day groups, respectively (RD - 3.2, 95%CI - 26.6 to 20.2). Most infections were of the respiratory tract (73/68.9%) and caused by carbapenem-resistant Enterobacterales (42/39.6%). The study was interrupted before reaching planned sample size due to low recruitment rate.
Conclusion: The OPTIMISE trial could not determine the non-inferiority of 7-day compared to 14-day therapy for severe infections caused by MDR-GNB due to early termination related to the low recruitment rate.
Trial registration: NCT05210387 on January 13, 2022.
Keywords: Acinetobacter baumannii; Enterobacterales; Klebsiella pneumoniae; Pseudomonas aeruginosa; Antimicrobial resistance; Antimicrobial therapy; Gram-negative bacteria.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol and amendments were approved by the research ethics committee (institutional review board, IRB) of the coordinating centre (Hospital Moinhos de Vento), as well as IRBs from all other participant sites. Written informed consent was obtained from the patients (or from a legal representative, if the patient was not capable of providing it at that moment). Consent for publication: Not applicable. Competing interests: BA received support for attending meetings and/or travel by MSD. G.M.N received payment for lectures for Pfizer and MSD and received support for attending meetings and/or travel by Pfizer. A.P.Z. is a research fellow of the National Council for Scientific and Technological Development (CNPq), Ministry of Science and Technology, Brazil. All other authors have no conflicts to declare.
Figures
References
-
- Stewardson AJ, Marimuthu K, Sengupta S, Allignol A, El-Bouseary M, Carvalho MJ, et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): a multinational prospective cohort study. Lancet Infect Dis. 2019;19:601–10. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
