

Analgesic efficacy and safety of erector spinae plane block versus serratus anterior plane block in breast surgery-a meta-analysis and systematic review of randomized controlled trials
- PMID: 39695870
- PMCID: PMC11657579
- DOI: 10.1186/s44158-024-00218-7
Analgesic efficacy and safety of erector spinae plane block versus serratus anterior plane block in breast surgery-a meta-analysis and systematic review of randomized controlled trials
Abstract
Background: Mastectomy and breast-conserving surgery are key interventions for breast cancer, a leading cause of cancer-related mortality in women. Many undergoing breast surgery experience postoperative pain compromising their functionality and quality of life. While multiple pain management strategies are available, evidence comparing the erector spinae (ESPB) and serratus anterior plane blocks (SAPB) for improving post-surgical pain management in breast cancer surgery patients is limited. Therefore, we investigated the efficacy and safety of these two regional anesthesia techniques.
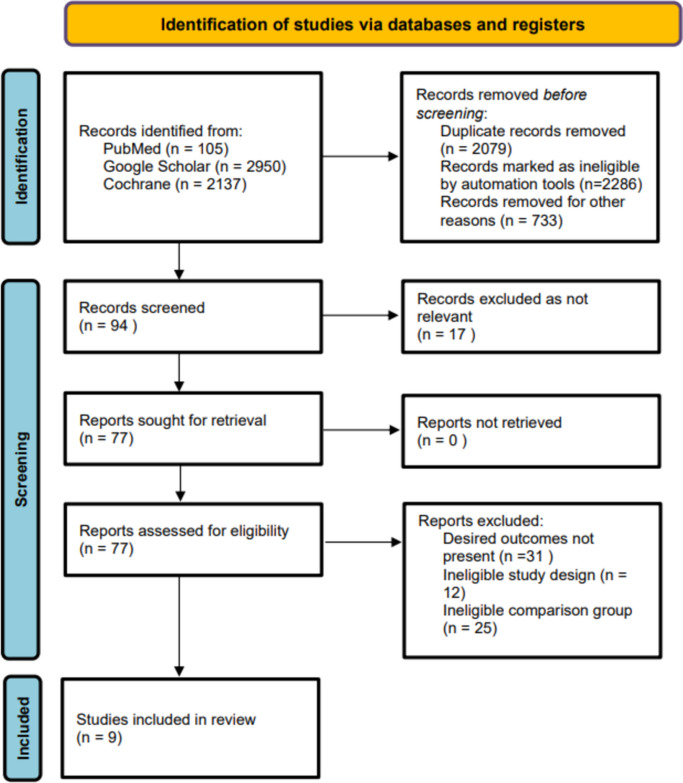
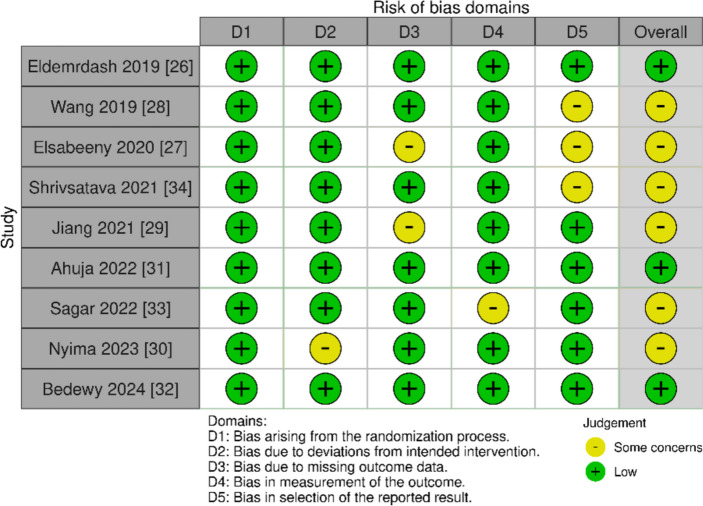
Methods: After PROSPERO registration, we systematically searched PubMed, Google Scholar, and Cochrane Library until May 2024. Risk ratios (RR) were calculated for dichotomous outcomes and standard mean differences (SMD) or mean differences (MD) were computed for continuous data. RevMan Review Manager 5.4.1 was used for the data analysis and generation of forest plots as well as funnel plots. The Cochrane Risk of Bias tool 2.0 (18) and Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) guidelines were used to appraise and evaluate the evidence (19).
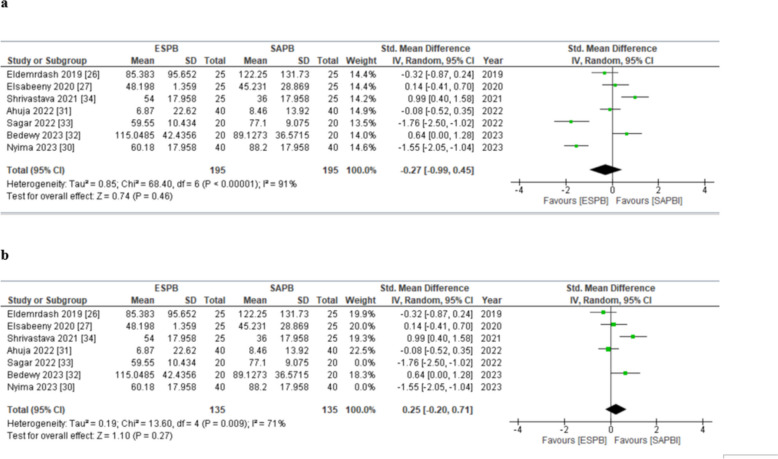
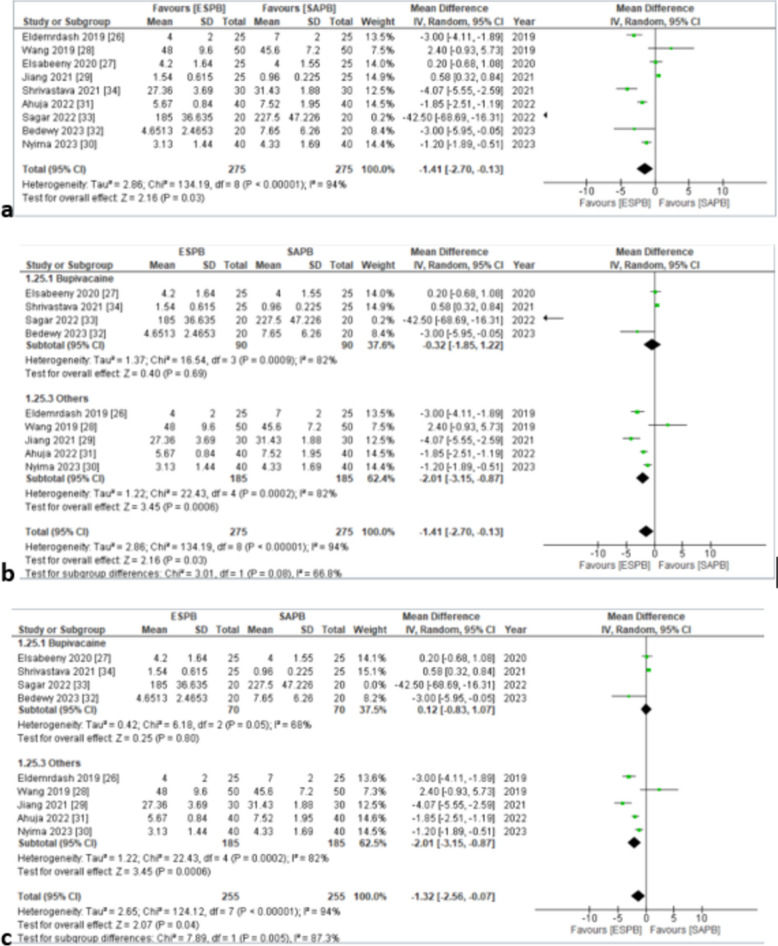
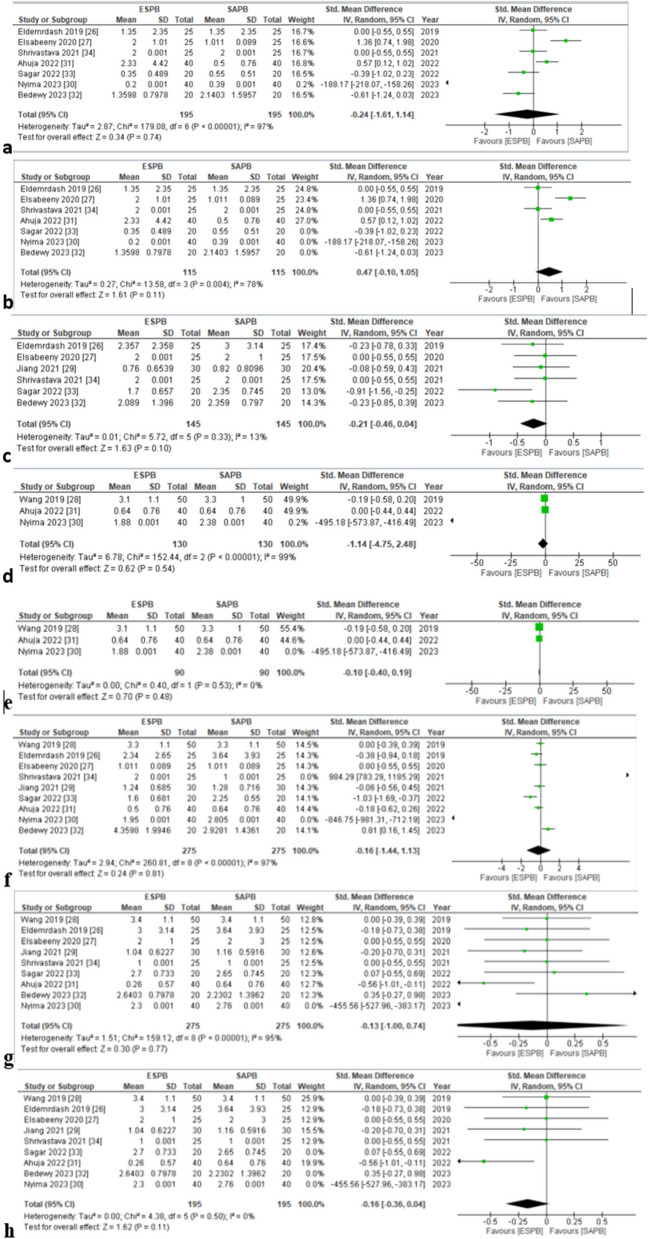
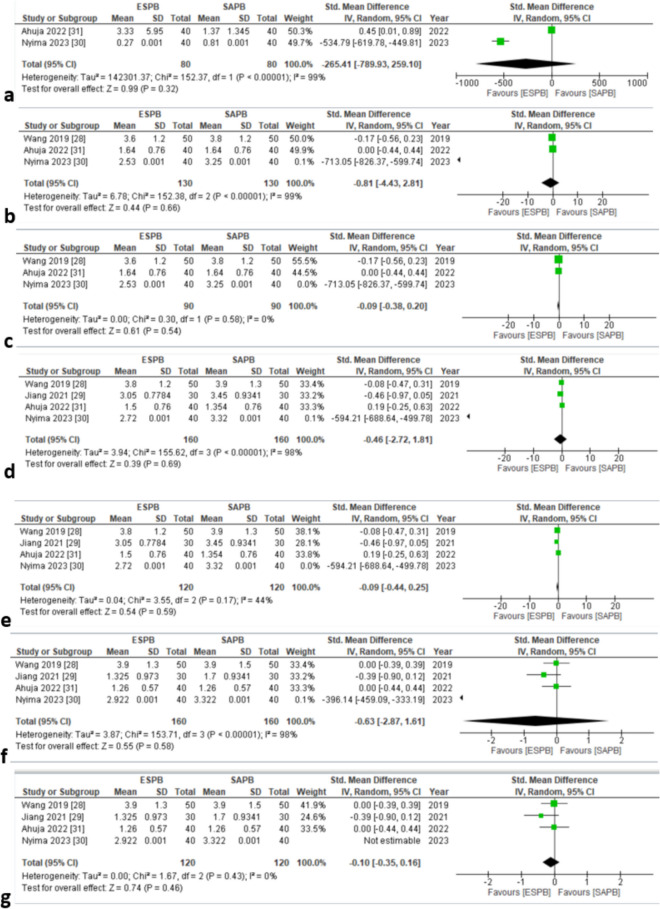
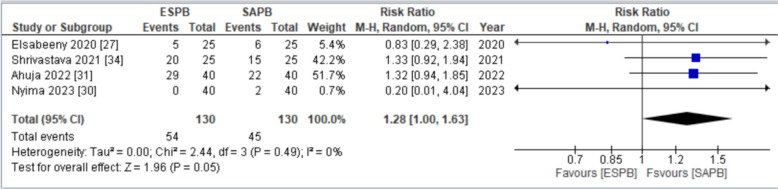
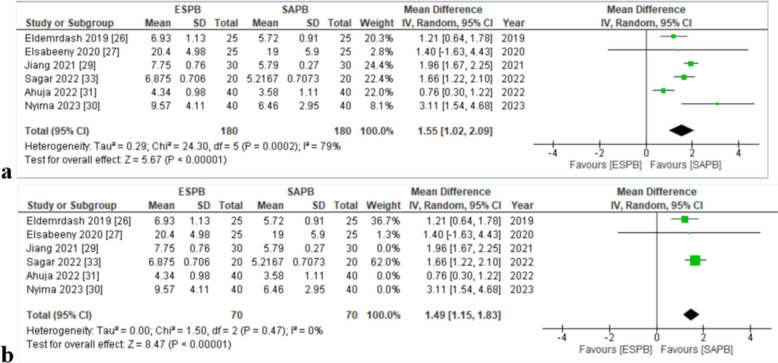
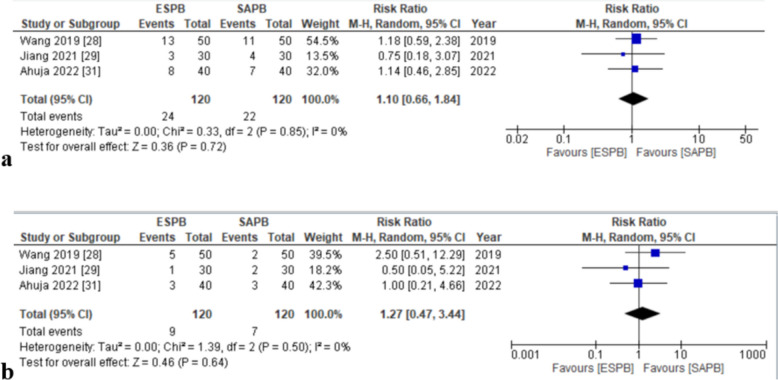
Results: A total of 9 randomized control trials enrolling 550 patients were included. Static pain scores at 0, 6, 8, 12, and 24 h after surgery, dynamic pain scores computed at 0, 8, 12, and 24 h after surgery and area under the curve (AUC) static pain score at all time points between 0 and 24 h (SMD (HKSJ 95% CI) - 0.27 [- 0.99, 0.45]) did not significantly vary with either plane block. Postoperative morphine consumption in the first 24 h and the number of patients requesting analgesia were significantly greater in those receiving SAPB [MD: - 1.41 (95% C.I. - 2.70, - 0.13), p = 0.03] and [RR: 1.28 (95% C.I. 1.00, 1.63), p = 0.05], respectively. The time to first postoperative analgesic use was significantly greater among those administered ESPB [MD: 1.55 h, (95% C.I. 1.02, 2.09), p < 0.01]. Patient satisfaction scores and the incidence of nausea and vomiting were similar across both groups.
Conclusions: While pain scores with either block are comparable, ESPB reduces postoperative morphine consumption and may be the favorable option in breast cancer patients undergoing surgery.
Keywords: Breast cancer surgery; ESPB; Postoperative pain; Regional anesthesia; SAPB.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Al –Gaithy ZK, Yaghmoor BE, Koumu MI, Alshehri KA, Saqah AA, Alshehri HZ. Trends of mastectomy and breast-conserving surgery and related factors in female breast cancer patients treated at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, 2009–2017: A retrospective cohort study. Ann Med Surg. 2019;41:47–52. - PMC - PubMed
-
- Ephrem Tadele Sedeta, Bilain Jobre, and Boris Avezbakiyev. Breast cancer: global patterns of incidence, mortality, and trends. | Journal of Clinical Oncology. Available from: https://ascopubs.org/doi/10.1200/JCO.2023.41.16_suppl.10528. Cited 2024 Jun 5.
-
- Chronic pain in female breast cancer survivors - prevalence, characteristics and contributing factors: a cross-sectional pilot study | BMC Women’s Health | Full Text. Available from: https://bmcwomenshealth.biomedcentral.com/articles/10.1186/s12905-023-02.... Cited 2024 Jun 5. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources