

Intraoperative extracorporeal support for lung transplant: a systematic review and network meta-analysis
- PMID: 39695889
- PMCID: PMC11658095
- DOI: 10.1186/s44158-024-00214-x
Intraoperative extracorporeal support for lung transplant: a systematic review and network meta-analysis
Abstract
Background: In the last decades, veno-arterial extracorporeal membrane oxygenation (V-A ECMO) has been gaining in popularity for intraoperative support during lung transplant (LT), being advocated for routinely use also in uncomplicated cases. Compared to off-pump strategy and, secondarily, to traditional cardiopulmonary bypass (CPB), V-A ECMO seems to offer a better hemodynamic stability and oxygenation, while data regarding blood product transfusions, postoperative recovery, and mortality remain unclear. This systematic review and network meta-analysis aims to evaluate the comparative efficacy and safety of V-A ECMO and CPB as compared to OffPump strategy during LT.
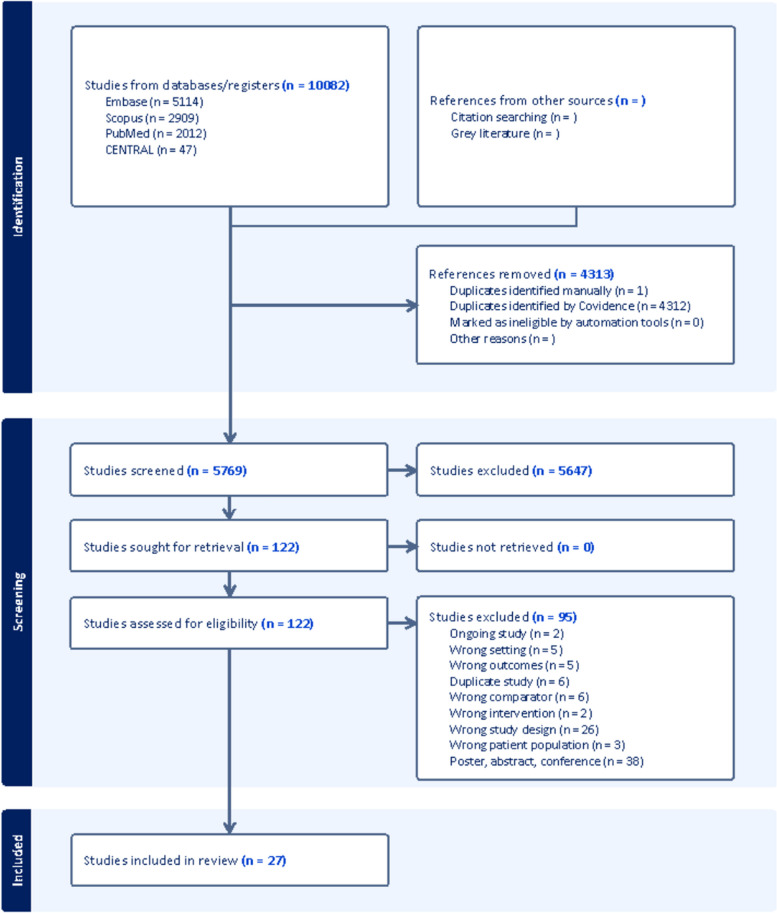
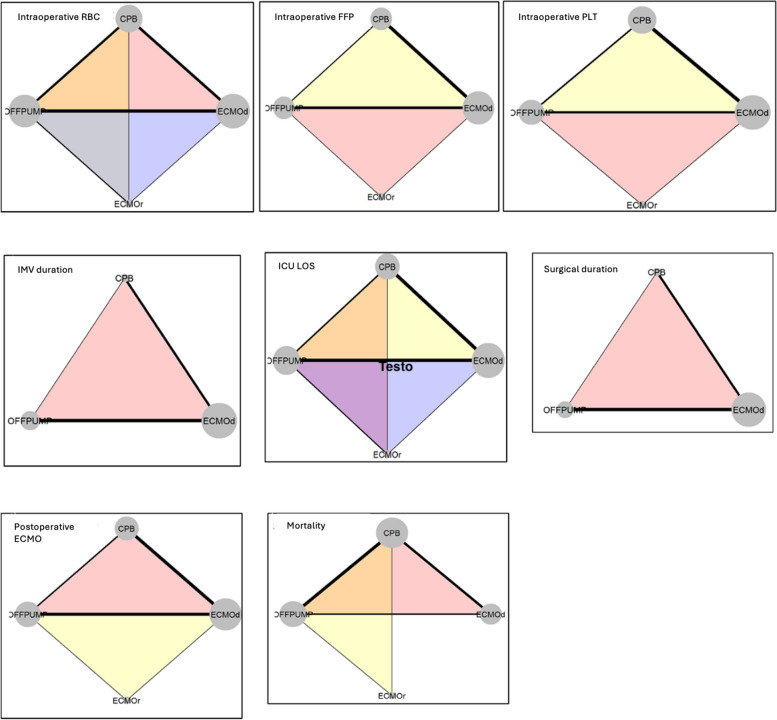
Methods: A comprehensive literature search was conducted across multiple databases (PubMed Embase, Cochrane, Scopus) and was updated in February 2024. A Bayesian network meta-analysis (NMA), with a fixed-effect approach, was performed to compare outcomes, such as intraoperative needing of blood products, invasive mechanical ventilation (IMV) duration, intensive care unit (ICU) length of stay (LOS), surgical duration, needing of postoperative ECMO, and mortality, across different supports (i.e., intraoperative V-A (default (d) or rescue (r)) ECMO, CPB, or OffPump).
Findings: Twenty-seven observational studies (6113 patients) were included. As compared to OffPump surgery, V-A ECMOd, V-A ECMOr, and CPB recorded a higher consumption of all blood products, longer IMV durations, prolonged ICU LOS, surgical duration, and higher mortalities. Comparing different extracorporeal supports, V-A ECMOd and, secondarily, V-A ECMOr overperformed CPB in nearly all above mentioned outcomes, except for RBC transfusions. The lowest rate of postoperative ECMO was recorded after OffPump surgery, while no differences were found comparing different extracorporeal supports. Finally, older age, male gender, and body mass index ≥ 25 kg/m2 negatively impacted on RBC transfusions, ICU LOS, surgical duration, need of postoperative ECMO, and mortality, regardless of the intraoperative extracorporeal support investigated.
Interpretation: This comparative network meta-analysis highlights that OffPump overperformed ECMO and CPB in all outcomes of interest, while, comparing different extracorporeal supports, V-A ECMOd and, secondarily, V-A ECMOr overperformed CPB in nearly all above mentioned outcomes, except for RBC transfusions. Older age, male gender, and higher BMI negatively affect several outcomes across different intraoperative strategies, regardless of the intraoperative extracorporeal support investigated. Future prospective studies are necessary to optimize and standardize the intraoperative management of LT.
Keywords: CPB; Cardiopulmonary bypass; ECMO; Extracorporeal membrane oxygenation; Lung transplant; Transplantation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Di Nardo M, Tikkanen J, Husain S, Singer LG, Cypel M, Ferguson ND et al (2022) Postoperative management of lung transplant recipients in the intensive care unit. Anesthesiology 136(3):482–499 - PubMed
-
- Khush KK, Cherikh WS, Chambers DC, Harhay MO, Hayes D, Hsich E et al (2019) The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: thirty-sixth adult heart transplantation report - 2019; focus theme: donor and recipient size match. J Heart Lung Transplant Off Publ Int Soc Heart Transplant 38(10):1056–1066 - PMC - PubMed
-
- Expert Consensus Panel, Hartwig M, van Berkel V, Bharat A, Cypel M, Date H et al (2023) The American Association for Thoracic Surgery (AATS) 2022 expert consensus document: the use of mechanical circulatory support in lung transplantation. J Thorac Cardiovasc Surg. 165(1):301–26 - PubMed
-
- Hoetzenecker K, Schwarz S, Muckenhuber M, Benazzo A, Frommlet F, Schweiger T et al (2018) Intraoperative extracorporeal membrane oxygenation and the possibility of postoperative prolongation improve survival in bilateral lung transplantation. J Thorac Cardiovasc Surg 155(5):2193-2206.e3 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials