

Clinical characteristics and risk factors of bacillary layer detachment in central serous chorioretinopathy: a comparative multicenter study
- PMID: 39695915
- PMCID: PMC11658337
- DOI: 10.1186/s40942-024-00612-x
Clinical characteristics and risk factors of bacillary layer detachment in central serous chorioretinopathy: a comparative multicenter study
Abstract
Background: Central serous chorioretinopathy (CSC) is marked by serous retinal detachments caused by fluid leakage from the retinal pigment epithelium, often associated with stress, psychiatric disorders and the use of corticosteroids. This study aims to investigate the clinical and systemic characteristics associated with BALAD in patients with CSC, comparing those with and without BALAD to clarify its function as a biomarker of CSC severity and improve diagnostic and treatment approaches.
Purpose: Compare the clinical characteristics, risk factors, and optical coherence tomography (OCT) findings in patients with Central Serous Chorioretinopathy (CSC) with and without Bacillary Layer Detachment (BALAD), and to identify the distinguishing features and associated conditions of CSC with BALAD.
Methods: This observational, retrospective, multicenter case-control study collected data from 12 retina centers worldwide on patients with central serous chorioretinopathy (CSC) from December 1, 2022, to April 1, 2023. CSC was defined by serous retinal detachment and fluid leakage through the retinal pigment epithelium. Patients underwent detailed evaluations, including OCT, and were classified as having acute or chronic CSC. Inclusion criteria included a CSC diagnosis with RPE leakage, BALAD confirmed by three authors, age over 18, and a detailed medical history from the 30 days before symptom onset. The study assessed visual acuity, choroidal thickness, psychiatric disorders, corticosteroid use, prior CSC treatments, and hyperreflective material on OCT.
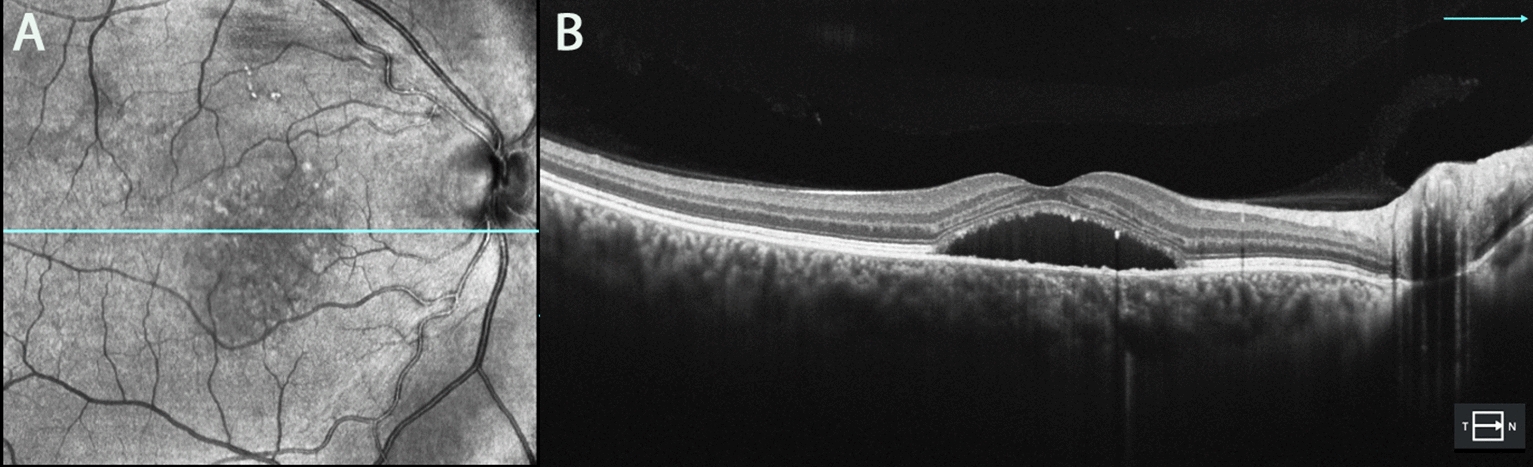
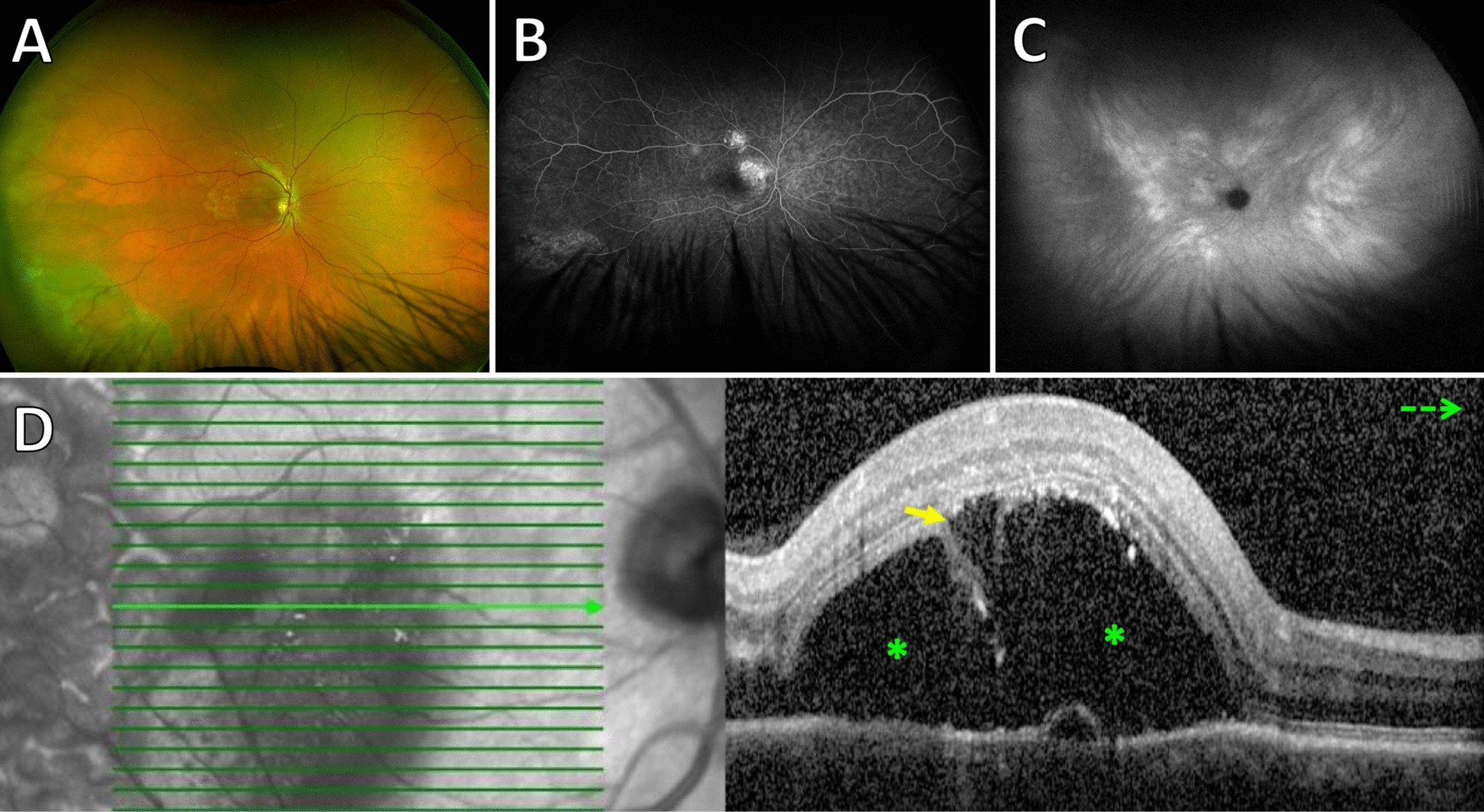
Results: Thirty-seven patients (40 eyes; mean age, 48.0 ± 11.9 years) had CSC and BALAD and were followed for a mean of 4.92 ± 6.65 months. The control group was comprised of 40 patients with CSC without BALAD (40 eyes; mean age, 48.2 ± 11.9 years). On clinical examination, BALAD was as a circular, yellowish macular lesion. On OCT, BALAD was a detachment of the ellipsoid zone with splitting of the photoreceptor inner segment. BALAD was associated with psychiatric disorders (p = 0.014), use of corticosteroids (p = 0.004), previous treatment for CSC (p = 0.041) and thickened choroid (p = 0.036).
Conclusions: BALAD in CSC differs from a typical CSC due to the presence of a circular, yellowish macular lesion, detachment of the ellipsoid zone, segmentation of the inner segment of the photoreceptor, a thicker choroid, the use of corticosteroids, and generally more aggressive previous treatments. These results suggest that BALAD may serve as a valuable biomarker for the severity of CSC and highlight the influence of inflammation and previous treatments.
Keywords: Bacillary layer detachment; Central serous chorioretinopathy; Inflammation; Photodynamic therapy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by all local ethics committee at each participating center. Consent for publication: Written informed consent was obtained from all patients in the study. Competing interests: AMC is editor-in-chief for IJRV, but he is not partipating of the peer review process.
Figures




References
LinkOut - more resources
Full Text Sources
Miscellaneous
