

Competing risks multi-state model for time-to-event data analysis of HIV/AIDS: a retrospective cohort national datasets, Ethiopia
- PMID: 39695972
- PMCID: PMC11654082
- DOI: 10.1186/s12879-024-10280-9
Competing risks multi-state model for time-to-event data analysis of HIV/AIDS: a retrospective cohort national datasets, Ethiopia
Abstract
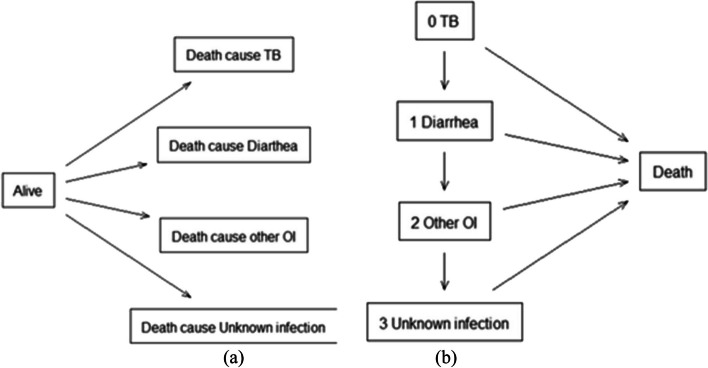
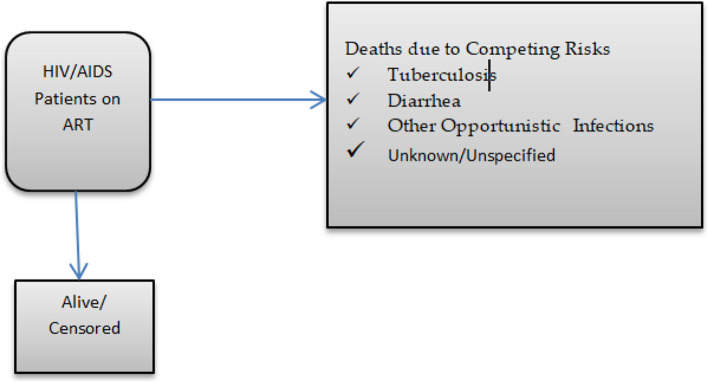
Introduction: Tuberculosis (TB) remains the most common opportunistic infection and leading cause of death among individuals living with HIV/AIDS in Ethiopia. Its significant impact on morbidity and mortality underscores the crucial link between these two diseases. While the advent of antiretroviral therapy (ART) has led to a dramatic decline in mortality rates among HIV/AIDS patients, TB continues to pose a substantial threat. This study aims to estimate the probability of death due to TB among HIV/AIDS patients on ART, considering the presence of various competing risks, including diarrhea, other infections, and unknown/unspecified causes. Also we have assessed the effects of prognostic factors on HIV/AIDS cause specific deaths, compared with the death from other competing risks, and exploring leading cause of death among HIV/AIDS patients on Antiretroviral Therapy.
Methods: Data from a retrospective research examining the effectiveness of antiretroviral therapy (ART) in Ethiopia were used in this investigation. The data came from medical records of patients who were part of the national ART program. A total of 39,590 records were gathered between October 2019 and March 2020 from all regions of Ethiopia as well as the administration cities of Addis Ababa and Dire Dawa. The study facilities were grouped using a multi-stage sample technique and simple random selection was used to select health facility and a person record from medical records. In the presence of the competing causes of death, Cause specific hazard, subdistribution hazard model and flexible parametric proportional hazard model have been used to assess the effect of covariates on the risk of death, with the cmprisk package in R4.3.2 software.
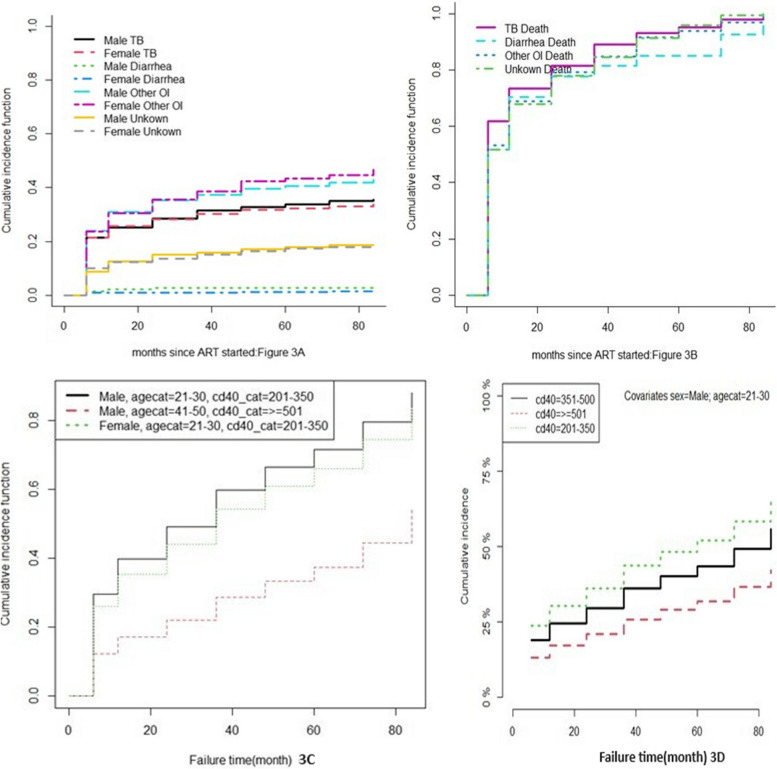
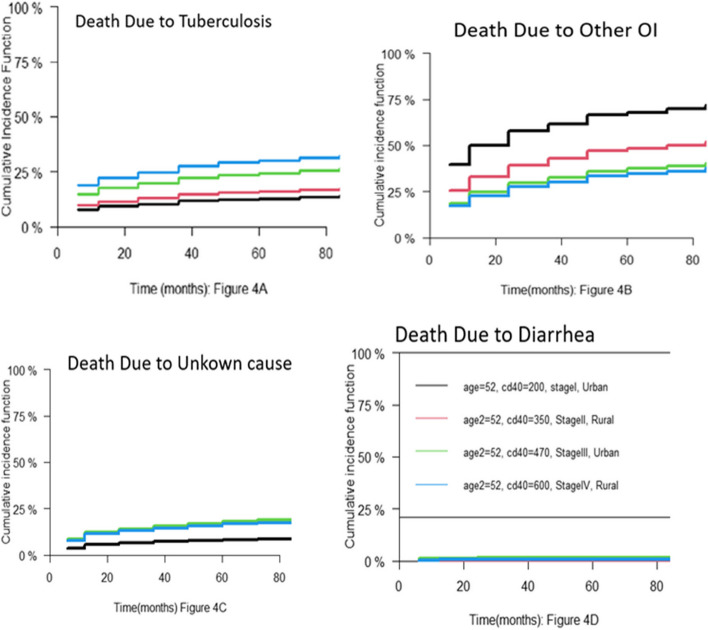
Results: Out of the total 1212 deaths, 542(44.7%) died competing with other opportunistic infection (TE-Esophageal Candidiasis, TO-oral, CT-CNS Toxoplasmosis, CM-Crypotococcal Meningitis…), 421 (34.7%) died due to tuberculosis and the remaining death were unknown/Not specified infection 222(18.3%) and diarrhea 27(2.2%). Rates of mortality caused by tuberculosis, competing with other opportunistic infection, diarrhea and unknown/Not specified were 3.5, 4.5, 0.2 and 1.8 per 1000 person-months, respectively. Having a higher CD4 count at diagnosis, responding to combination antiretroviral treatment (cART) six months after start, and having prophylactic treatment for pneumocystis pneumonia (PCP) decreased the risk of tuberculosis, other opportunistic infections, and unidentified and diarrheal causes of death. However, older age, late HIV.AIDS diagnosis, and the last HIV/AIDS WHO clinical stages increased the hazard of tuberculosis and other opportunistic disease mortality. Additionally, male gender, older age and last HIV clinical stages increased the mortality HIV/AIDS patients.
Conclusion: The findings of this study demonstrated that TB, an opportunistic infection, was the primary cause of death in HIV/AIDS patients, despite the presence of several competing risks, such as diarrhea, other infections, and an undetermined or unclear cause. It's important to use effective techniques to quickly detect those who have HIV or AIDS and provide them with care and treatment to increase their chances of surviving.
Keywords: AIDS; Competing risk; Cumulative Incidence Function; ·Cause-specific hazard; ·Sub-distribution hazard.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical clearance was initially obtained back in June/July 2019 from AHRI/ALERT Ethics Review Committee [P048/18]. Consecutively, before dispatching the team to the different regions, a formal official approval and support letter describing the purposes of the study was written from Federal MoH to the respective Regional health bureaus and in turn to each zonal offices and hospitals and then from Zonal Health Bureaus to the Woreda Health Offices before reaching the health facilities. The declaration of Helsinki and national ethical guidelines were followed in the conduct of the study. Consent for publication: Not Applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- W. H. Organization(WHO), World Health Organization HIV and AIDS 2023. Accessed from https://www.who.int/news-room/fact-sheets/detail/hiv-aids/key/facts. 2023, pp. 1–23.
-
- Ethiopian Public Health Institute, “HIV Related Estimates and Projections in Ethiopia for the Year 2021–2022 August 2022 Addis Ababa,” Gmf. pp. 1–32, 2023. Available: https://ephi.gov.et/wp-content/uploads/2021/02/HIV-Estimates-and-project....
-
- R. A. B., Yeh C-M. Institute of Mathematical Statistics is collaborating with JSTOR to digitize, preserve, and extend access to The Annals of Statistics. Ann Stat. 1980;8(4):883–93 www.jstor.org.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
