

The prehospital paediatric emergency care burden managed by a public ambulance service in the Western Cape, South Africa
- PMID: 39695979
- PMCID: PMC11658289
- DOI: 10.1186/s12873-024-01146-z
The prehospital paediatric emergency care burden managed by a public ambulance service in the Western Cape, South Africa
Abstract
Background: Paediatric mortality rates in low- and middle-income countries account for over 80% of the global burden. In South Africa, one in every 33 children will not reach the age of five. Despite the high mortality rate, there is a paucity of data describing the prehospital paediatric under-five emergency care burden in South Africa. Such data are essential to inform the development of local prehospital emergency care guidelines and targeted prevention strategies.
Aim: This study describes the prehospital paediatric under-five emergency care burden managed by the Western Cape Government Health and Wellness (WCGHW) Emergency Medical Services (EMS) in South Africa.
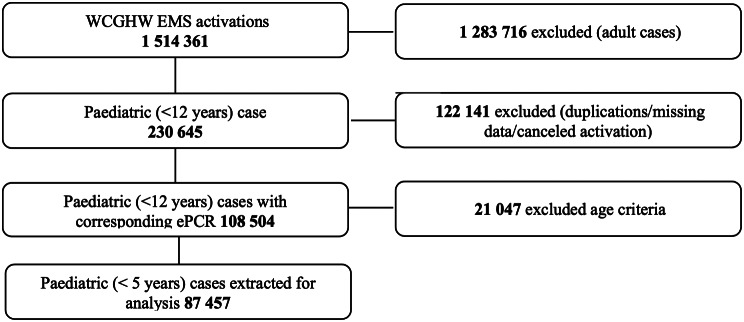
Methods: A retrospective review of the prehospital records was conducted, extracting epidemiological and clinical data from the WCGHW EMS patient record database. The review included all paediatric cases under-five, managed between 1 January 2022 and 31 December 2023, in the Western Cape of South Africa.
Results: In the 87 457 cases, there was a similar distribution between the primary cases (50.7%) and interfacility transfers (49.3%). Most activations emanated from rural areas (47 980, 54.9%), with respiratory emergencies (30 934, 35.4%), non-cardiac pain (11 381, 13.0%) and trauma (10 831,12.4%) being the most common presenting complaints. Most cases were prioritised as priority 2 (46 034, 52.6%), with most of these being older children between one and five years old (29 008, 63.0). Low acuity cases accounted for 67.2% (58 818) of the sample, with the highest mortality occurring between 29 days and 12 months (190, 52.9.%). Most patients spent less than one hour in the prehospital setting (64 431, 73.7%), with advanced airway management (748, 43.1%) being the most common airway intervention.
Conclusion: This first description of the prehospital paediatric under-five emergency care burden managed by the WCGHW EMS reveals a unique burden, particularly regarding the high interfacility transfer rates. As illustrated in graphical abstract, these findings underscore critical considerations for healthcare planners and the prehospital training environment. Future research among this population should focus on characterising the reasons for the high interfacility transfer rates through assessments of healthcare access, EMS care quality and post-EMS follow-up.
Keywords: Emergency medical services; Epidemiology; Low to middle-income country (LMIC); Paediatric emergencies; Prehospital paediatric burden; South Africa.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethics approval was obtained through the Cape Peninsula University of Technology Health and Wellness Sciences Research Ethics Committee (CPUT/HWS-REC 2024/H8) and the WCGHW EMS (WC_202405_040). This study involved the retrospective analysis of de-identified secondary data, routinely captured and stored on the WCGHW EMS patient record database, the Cape Peninsula University of Technology Health and Wellness Sciences Research Ethics Committee waived the need for informed consent. All procedures were followed in accordance with the Helsinki Declaration of 1975. Consent for publication: None applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
The triage performance of emergency medical dispatch prioritisation compared to prehospital on-scene triage in the Western Cape Province of South Africa.BMC Emerg Med. 2025 Mar 6;25(1):42. doi: 10.1186/s12873-025-01198-9. BMC Emerg Med. 2025. PMID: 40050736 Free PMC article.
-
Defining and improving the role of emergency medical services in Cape Town, South Africa.Emerg Med J. 2016 Aug;33(8):557-61. doi: 10.1136/emermed-2015-205177. Epub 2016 Feb 4. Emerg Med J. 2016. PMID: 26848162
-
Out-of-hospital cardiac arrests in the city of Cape Town, South Africa: a retrospective, descriptive analysis of prehospital patient records.BMJ Open. 2021 Aug 16;11(8):e049141. doi: 10.1136/bmjopen-2021-049141. BMJ Open. 2021. PMID: 34400458 Free PMC article.
-
Child and adolescent mortality associated with pesticide toxicity in Cape Town, South Africa, 2010-2019: a retrospective case review.BMC Public Health. 2023 Apr 28;23(1):792. doi: 10.1186/s12889-023-15652-5. BMC Public Health. 2023. PMID: 37118778 Free PMC article. Review.
-
EMS Systems in Lower-Middle Income Countries: A Literature Review.Prehosp Disaster Med. 2017 Feb;32(1):64-70. doi: 10.1017/S1049023X1600114X. Epub 2016 Dec 12. Prehosp Disaster Med. 2017. PMID: 27938449 Review.
References
-
- UNICEF. UNICEF DATA. 2024 [cited 2024 Jun 20]. South Africa (ZAF) - Demographics, Health & Infant Mortality. https://data.unicef.org/country/zaf/
-
- Mowafi H, Dworkis D, Bisanzo M, Hansoti B, Seidenberg P, Obermeyer Z, et al. Making recording and analysis of chief complaint a priority for global emergency care research in low-income countries. Acad Emerg Med off J Soc Acad Emerg Med. 2013;20(12):1241–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
