

Leopard spot retinopathy represents the initial sign of rhegmatogenous retinal detachment in children: a report of two cases
- PMID: 39696057
- PMCID: PMC11658082
- DOI: 10.1186/s12886-024-03802-1
Leopard spot retinopathy represents the initial sign of rhegmatogenous retinal detachment in children: a report of two cases
Abstract
Background: Leopard spots can appear in a variety of diseases; however, they are extremely rare in children with rhegmatogenous retinal detachment. This study presents two such rare cases in which leopard spot retinopathy was the initial manifestation of rhegmatogenous retinal detachment.
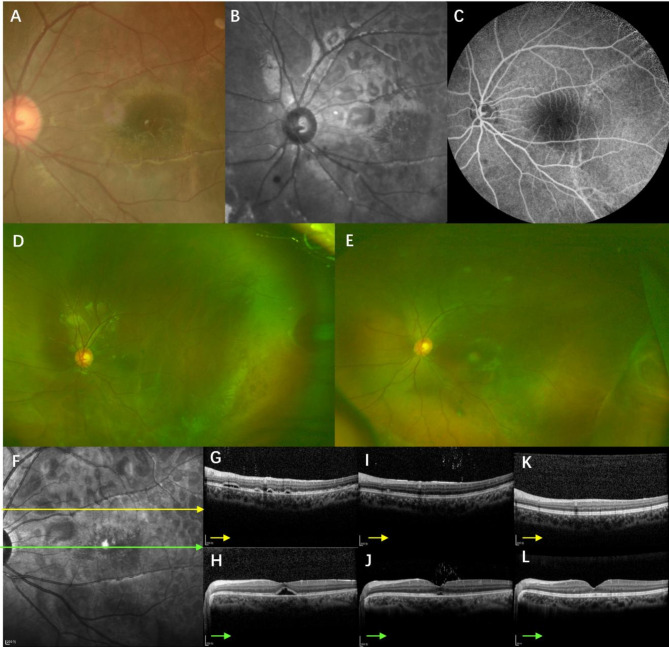
Case presentation: Case 1 involved a 4-year-old boy had previously been diagnosed with left eye uveitis and received systemic steroid therapy at a local hospital, but symptoms persisted. Extensive leopard-spot changes were observed in the posterior pole of the left eye and optical coherence tomography (OCT) showed multifocal, shallow retinal detachment in the left eye. Case 2 involved a 16-year-old girl who visited for decreased vision in her right eye. Examination of the right eye revealed leopard-spot changes at the posterior pole and a retinal hole in the fundus; multifocal retinal detachment was noted on OCT. In both cases, subretinal fluid was significantly absorbed after retinal laser photocoagulation or scleral buckling, with no recurrence of retinal detachment at late follow-up.
Conclusions: When leopard-spot changes are observed, the fundus must be carefully examined for any potential retinal holes, especially in pediatric patients.
Keywords: Bilateral diffuse uveal melanocytic proliferation (BDUMP); Leopard spot; Primary intraocular lymphoma (PIOL); Rhegmatogenous retinal detachment.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Written informed consent for publication was obtained from the patients and their guardians. Competing interests: The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
