The performance of JAM3/PAX1 methylation in the diagnosis of high-grade squamous intraepithelial lesions for women with high-risk HPV infection
- PMID: 39696066
- PMCID: PMC11658199
- DOI: 10.1186/s12885-024-13299-y
The performance of JAM3/PAX1 methylation in the diagnosis of high-grade squamous intraepithelial lesions for women with high-risk HPV infection
Abstract
Objective: To assess the clinical value of DNA methylation measurement in exfoliated cervical cells for distinguishing high-grade squamous intraepithelial lesions (HSIL) from other cervical abnormalities.
Methods: A total of 276 patients were enrolled, and general clinical information was collected. Exfoliated cervical cells were obtained to assess human papillomavirus (HPV) infection, conduct ThinPrep cytology tests (TCT), and measure methylation levels of JAM3 (△CtJ) and PAX1 (△CtP). Logistic regression was performed to identify factors significantly associated with HSIL diagnosis. A conditional inference tree model and the area under the curve (AUC) were employed to evaluate the efficacy of JAM3 and PAX1 methylation in detecting HSIL.
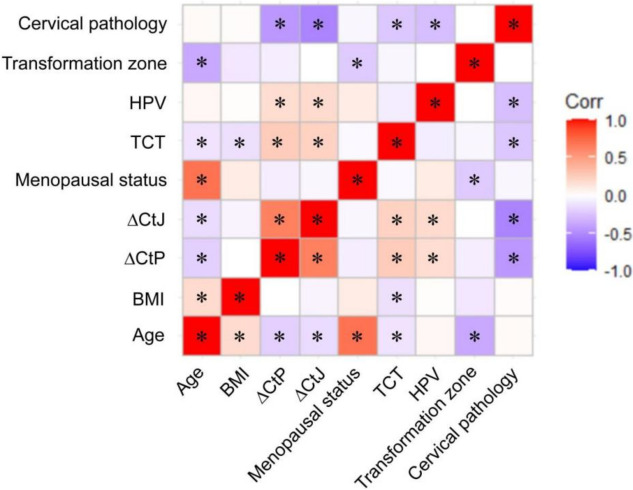
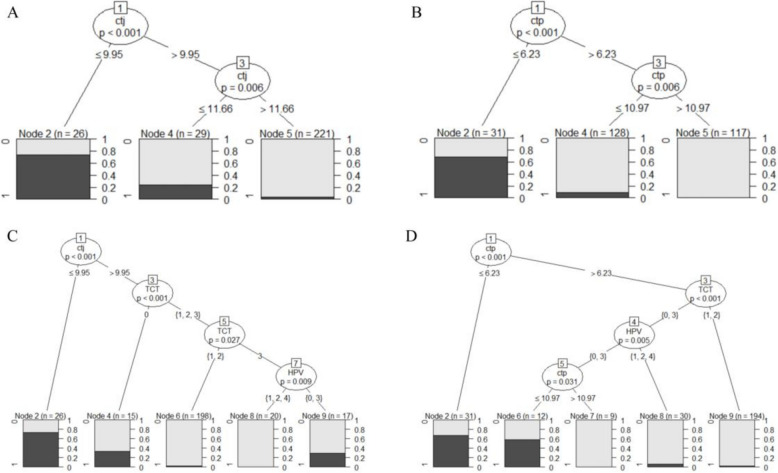
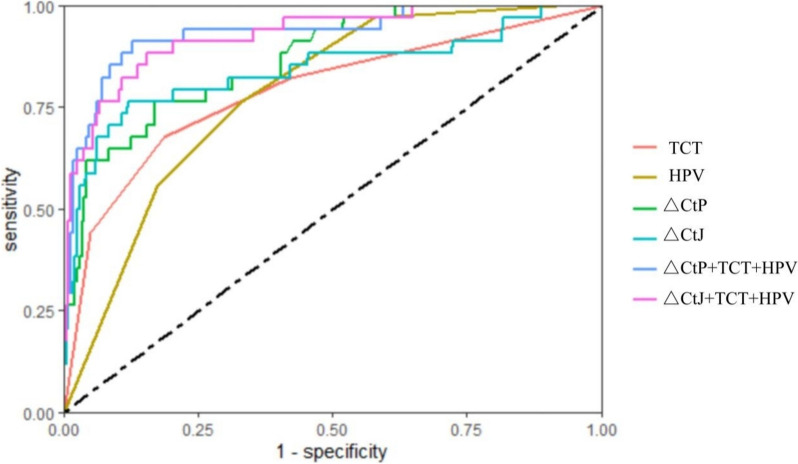
Results: Independent risk factors for HSIL diagnosis included △CtJ, △CtP, atypical squamous cells of undetermined significance (ASCUS), and HPV16 infection. The conditional inference tree indicated that 96.4% of patients were non-HSIL when △CtJ > 11.66, and 99.1% were non-HSIL when △CtP > 10.97. The diagnostic performance of △CtJ/△CtP surpassed that of TCT/HPV alone. Among six methods, the combination of △CtP, TCT, and high-risk HPV (hr-HPV) testing achieved the highest sensitivity (91.2%), positive predictive value (50.0%), negative predictive value (98.6%), and AUC (0.932).
Conclusion: In women with hr-HPV infection, DNA methylation analysis of cervical cytology outperformed traditional TCT or HPV testing. The combination of △CtP with TCT and HPV may offer the most accurate screening approach for HSIL.
Keywords: JAM3; PAX1; DNA methylation; High-grade squamous intraepithelial lesions; Hr-HPV.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the Third Xiangya Hospital of Central South University (No. 23137). All participants provided written informed consent. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures