

Early prediction of mortality upon intensive care unit admission
- PMID: 39696315
- PMCID: PMC11656927
- DOI: 10.1186/s12911-024-02807-6
Early prediction of mortality upon intensive care unit admission
Abstract
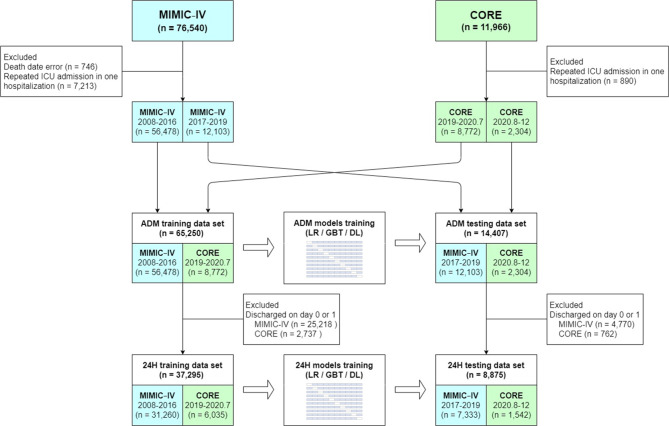
Background: We aimed to develop and validate models for predicting intensive care unit (ICU) mortality of critically ill adult patients as early as upon ICU admission.
Methods: Combined data of 79,657 admissions from two teaching hospitals' ICU databases were used to train and validate the machine learning models to predict ICU mortality upon ICU admission and at 24 h after ICU admission by using logistic regression, gradient boosted trees (GBT), and deep learning algorithms.
Results: In the testing dataset for the admission models, the ICU mortality rate was 7%, and 38.4% of patients were discharged alive or dead within 1 day of ICU admission. The area under the receiver operating characteristic curve (0.856, 95% CI 0.845-0.867) and area under the precision-recall curve (0.331, 95% CI 0.323-0.339) were the highest for the admission GBT model. The ICU mortality rate was 17.4% in the 24-hour testing dataset, and the performance was the highest for the 24-hour GBT model.
Conclusion: The ADM models can provide crucial information on ICU mortality as early as upon ICU admission. 24 H models can be used to improve the prediction of ICU mortality for patients discharged more than 1 day after ICU admission.
Keywords: Critically ill; Intensive care; Mortality; Prediction.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: MIMIC-IV database usage was approved by the Institutional Review Boards of Massachusetts Institute of Technology (no. 0403000206) and Beth Israel Deaconess Medical Center (2001-P-001699/14). CORE database used in our study was approved by the Research Ethics Committee (REC) of the National Taiwan University Hospital (REC no. 202004016RINB). Because this study was a secondary analysis of fully anonymized data, individual patient consent was not required. All investigations were performed in accordance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Cardona M, Dobler CC, Koreshe E, et al. A catalogue of tools and variables from crisis and routine care to support decision-making about allocation of intensive care beds and ventilator treatment during pandemics: scoping review. J Crit Care. 2021;66:33–43. - PubMed
-
- Lim SC, Fok AC, Ong YY. Patient outcome and intensive care resource allocation using apache ii. Singap Med J. 1996;37:488–91. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
