

Contribution and evolution of respiratory muscles function in weaning outcome of ventilator-dependent patients
- PMID: 39696360
- PMCID: PMC11654075
- DOI: 10.1186/s13054-024-05172-y
Contribution and evolution of respiratory muscles function in weaning outcome of ventilator-dependent patients
Abstract
Background: The present study was designed to investigate the evolution and the impact of respiratory muscles function and limb muscles strength on weaning success in prolonged weaning of tracheotomized patients. The primary objective was to determine whether the change in respiratory muscles function and limb muscles strength over the time is or is not associated with weaning success.
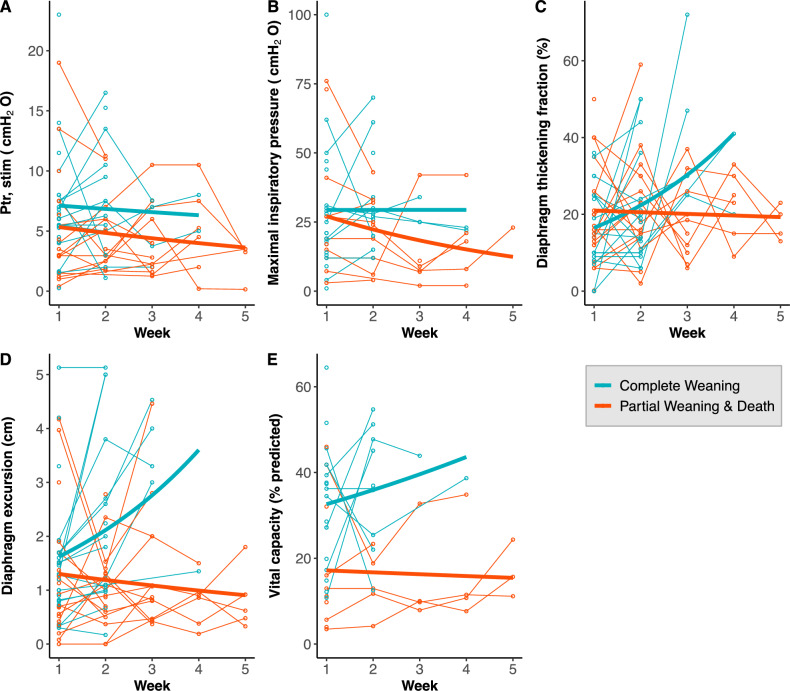
Methods: Tracheotomized patients who were ventilator dependent upon admission at a weaning center were eligible. Diaphragm function was assessed with the phrenic nerve stimulation technique and with ultrasound to measure the diaphragm thickening fraction (TFdi) and diaphragm excursion (EXdi). Global respiratory muscle function was assessed with the maximal inspiratory pressure (MIP) and the forced vital capacity (FVC). Limb muscle strength was measured with the Medical Research Council Score (MRC). Measurements were made on a weekly basis. Patients were compared according to their outcome at discharge: complete weaning, partial weaning or death.
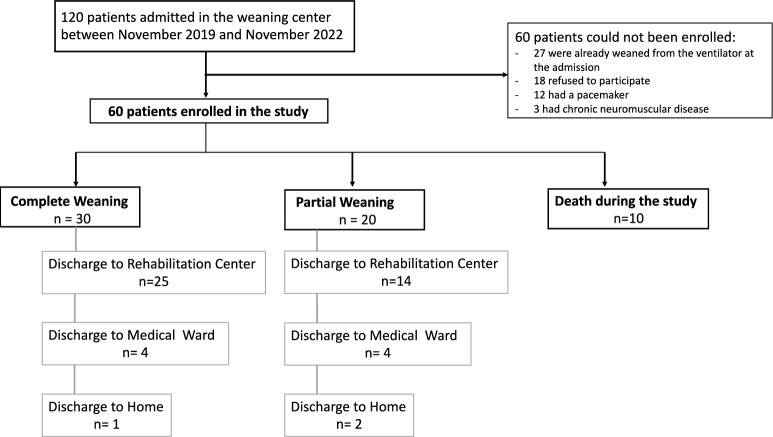
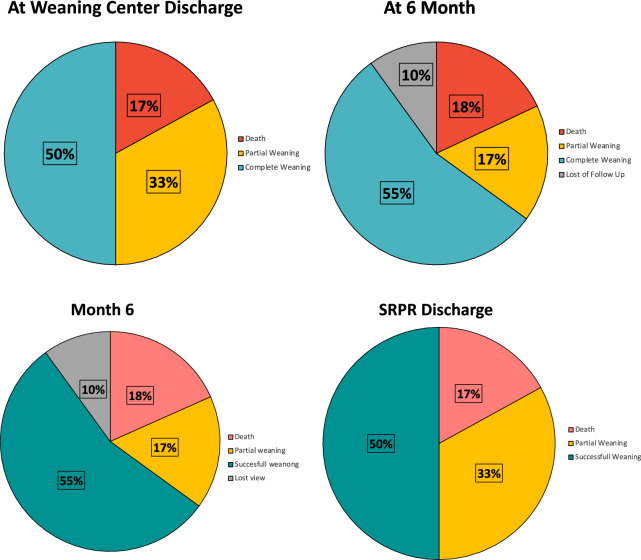
Results: Among the 60 patients who were enrolled, 30 patients finally achieved complete weaning, 20 had partial weaning and 10 died. At 6 months, 6 patients were lost of follow-up, 33 achieved complete weaning, 10 had partial weaning and 11 died. In median, 2 (1-9) assessments were performed per patient. Diaphragm dysfunction was present in all patients with a median Ptr,stim of 5.5 cmH2O (3.0-7.5). Ptr,stim, MIP, TFdi and EXdi at admission were not different between patients who achieved complete weaning and their counterparts. At discharge of the weaning center, MIP, Ptr,stim and EXdi significantly increased in patients who achieved complete weaning. The MRC score significantly increased only in patients with complete weaning. At discharge, diaphragm dysfunction was highly prevalent even in patients with complete weaning (Ptr,stim < 11 cmH2O in n = 11 (37%)).
Conclusion: Respiratory muscle function and limb muscles strength are severely impaired in patients with prolonged weaning from mechanical ventilation. Significant improvement of diaphragm ultrasound indices was associated with successful weaning from mechanical ventilation and ICU-acquired weakness upon admission was significantly associated with good outcome suggesting that it was an amendable determinant of weaning failure in this population.
Trial registration: ClinicalTrials.gov NCT03676998.
Keywords: Diaphragm dysfunction; Diaphragm ultrasound; ICU-acquired weakness; Mechanical ventilation; Prolonged weaning.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Research Ethics Committee of Sorbonne University approved the study (CER 2020-36). Oral information about the study was given to patients or relatives. Consent for publication: Not applicable. Competing interests: Martin Dres received fees from Lungpacer (expertise, lectures). A Demoule reports personal fees from Medtronic, grants, personal fees and non-financial support from Philips, personal fees from Baxter, personal fees from Hamilton, personal fees and non-financial support from Fisher & Paykel, grants from French Ministry of Health, personal fees from Getinge, grants and personal fees from Respinor, grants and non-financial support from Lungpacer, outside the submitted work. The other authors have no conflicts of interest to declare.
Figures

References
-
- Goligher EC, Ferguson ND, Brochard LJ. Clinical challenges in mechanical ventilation. Lancet. 2016;387(10030):1856–66. - PubMed
-
- Pham T, Heunks L, Bellani G, Madotto F, Aragao I, Beduneau G, et al. Weaning from mechanical ventilation in intensive care units across 50 countries (WEAN SAFE): a multicentre, prospective, observational cohort study. Lancet Respir Med. 2023;S2213–2600(22):00449. - PubMed
-
- Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010;38(10):1947–53. - PubMed
-
- Puthucheary ZA, Rawal J, McPhail M, Connolly B, Ratnayake G, Chan P, et al. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310(15):1591–600. - PubMed
-
- De Jonghe B, Sharshar T, Lefaucheur JP, Authier FJ, Durand-Zaleski I, Boussarsar M, et al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA. 2002;288(22):2859–67. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
