

Asciminib add-on to imatinib demonstrates sustained high rates of ongoing therapy and deep molecular responses with prolonged follow-up in the ASC4MORE study
- PMID: 39696526
- PMCID: PMC11657281
- DOI: 10.1186/s13045-024-01642-6
Asciminib add-on to imatinib demonstrates sustained high rates of ongoing therapy and deep molecular responses with prolonged follow-up in the ASC4MORE study
Abstract
Background: Up to 65% of patients with chronic myeloid leukemia (CML) who are treated with imatinib do not achieve sustained deep molecular response, which is required to attempt treatment-free remission. Asciminib is the only approved BCR::ABL1 inhibitor that Specifically Targets the ABL Myristoyl Pocket. This unique mechanism of action allows asciminib to be combined with adenosine triphosphate-competitive tyrosine kinase inhibitors to prevent resistance and enhance efficacy. The phase II ASC4MORE trial investigated the strategy of adding asciminib to imatinib in patients who have not achieved deep molecular response with imatinib.
Methods: In ASC4MORE, 84 patients with CML in chronic phase not achieving deep molecular response after ≥ 1 year of imatinib therapy were randomized to asciminib 40 or 60 mg once daily (QD) add-on to imatinib 400 mg QD, continued imatinib 400 mg QD, or switch to nilotinib 300 mg twice daily.
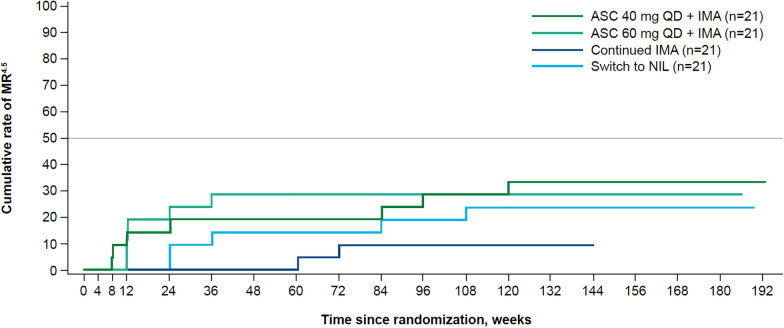
Results: More patients in the asciminib 40- and 60-mg QD add-on arms (19.0% and 28.6%, respectively) achieved MR4.5 (BCR::ABL1 ≤ 0.0032% on the International Scale) at week 48 (primary endpoint) than patients in the continued imatinib (0.0%) and switch to nilotinib (4.8%) arms. Fewer patients discontinued asciminib 40- and 60-mg QD add-on treatment (14.3% and 23.8%, respectively) than imatinib (76.2%, including crossover patients) and nilotinib (47.6%). Asciminib add-on was tolerable, with rates of AEs and AEs leading to discontinuation less than those with nilotinib, although higher than those with continued imatinib (as expected in these patients who had already been tolerating imatinib for ≥ 1 year). No new or worsening safety signals were observed with asciminib add-on vs the known asciminib monotherapy safety profile.
Conclusions: Overall, these results support asciminib add-on as a treatment strategy to help patients with CML in chronic phase stay on therapy to safely achieve rapid and deep response, although further investigation is needed before this strategy is incorporated into clinical practice.
Trial registration: NCT03578367.
Keywords: ASC4MORE; Add-on; Asciminib; CML; Combination; Deep molecular response; Imatinib; Tyrosine kinase inhibitors.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The protocol was approved by the sites' institutional review boards and conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent. Consent for publication: Not applicable; no individual patient data are included. Competing interests: TPH received research funding from Novartis, and Bristol Myers Squibb, and consultancy fees from Novartis, Takeda, Terns Pharmaceuticals, Enliven Therapeutics, and Ascentage Pharma. JG has received payment for consultancy from Novartis and Incyte. He is a committee member of the European Hematologic Association. He reports grants to his patient advocacy organization from Novartis, Pfizer, Bristol Myers Squibb, Incyte, Takeda, and Terns Pharmaceuticals. D-WK received research funding from Novartis, Bristol Myers Squibb, Enliven, Korea Otsuka, Il-Yang, and PharmaEssentia; honoraria from Novartis, Bristol Myers Squibb, Enliven, Krea Otsuka, and Il-Yang; and speaker bureau fees from Novartis, Bristol Myers Squibb, Korea Otsuka, and Il-Yang. EL received personal fees from Novartis, and Pfizer and is a member of speakers bureaus for Novartis, Pfizer, and Fusion Pharma. JM received research funding from BeiGene. AT received personal fees from Novartis, Pfizer, and R-Pharma and is a member of the speakers bureaus for Novartis, Pfizer, and R-Pharma. JEC received research funding from AbbVie, Ascentage Pharma, Novartis, and Sun Pharma and consultancy fees from Lilly, Nerviano, Novartis, Pfizer, Rigel, Sun Pharma, Syndax, and Biopath Holdings. He holds stock options in and is a board member of Biopath Holdings. BN, and SQ are employees of Novartis. APC and SK are employees and shareholders of Novartis stock. GS declares no competing interests.
Figures







References
-
- Shah NP, Bhatia R, Altman JK, Amaya M, Begna KH, Berman E, et al. Chronic myeloid leukemia, version 2.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2024;22(1):43–69. - PubMed
-
- Branford S, Seymour JF, Grigg A, Arthur C, Rudzki Z, Lynch K, Hughes T. BCR-ABL messenger RNA levels continue to decline in patients with chronic phase chronic myeloid leukemia treated with imatinib for more than 5 years and approximately half of all first-line treated patients have stable undetectable BCR-ABL using strict sensitivity criteria. Clin Cancer Res. 2007;13(23):7080–5. - PubMed
-
- Colombat M, Fort MP, Chollet C, Marit G, Roche C, Preudhomme C, et al. Molecular remission in chronic myeloid leukemia patients with sustained complete cytogenetic remission after imatinib mesylate treatment. Haematologica. 2006;91(2):162–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
