

Impact of board-certified intensive care training facilities on choice of adjunctive therapies and prognosis of severe respiratory failure: a nationwide cohort study
- PMID: 39696527
- PMCID: PMC11658443
- DOI: 10.1186/s40560-024-00766-8
Impact of board-certified intensive care training facilities on choice of adjunctive therapies and prognosis of severe respiratory failure: a nationwide cohort study
Abstract
Background: Patients with severe respiratory failure have high mortality and need various interventions. However, the impact of intensivists on treatment choices, patient outcomes, and optimal intensivist staffing patterns is unknown. In this study, we aimed to evaluate treatments and clinical outcomes for patients at board-certified intensive care training facilities compared with those at non-certified facilities.
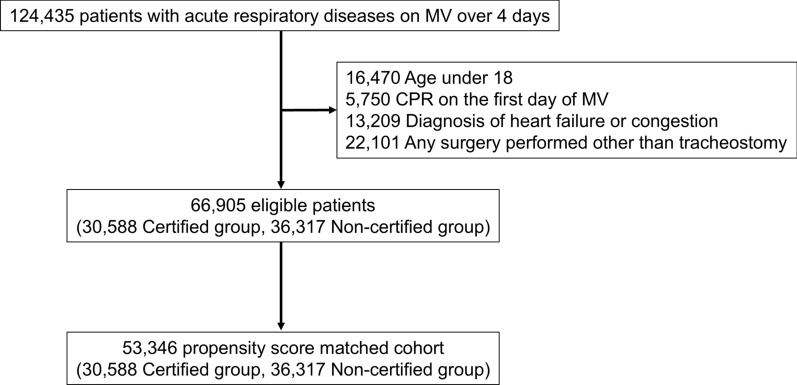
Methods: This retrospective cohort study used Japan's nationwide in-patient database from 2016 to 2019 and included patients with non-operative severe respiratory failure who required mechanical ventilation for over 4 days. Treatments and in-hospital mortality were compared between board-certified intensive care facilities requiring at least one intensivist and non-certified facilities using propensity score matching.
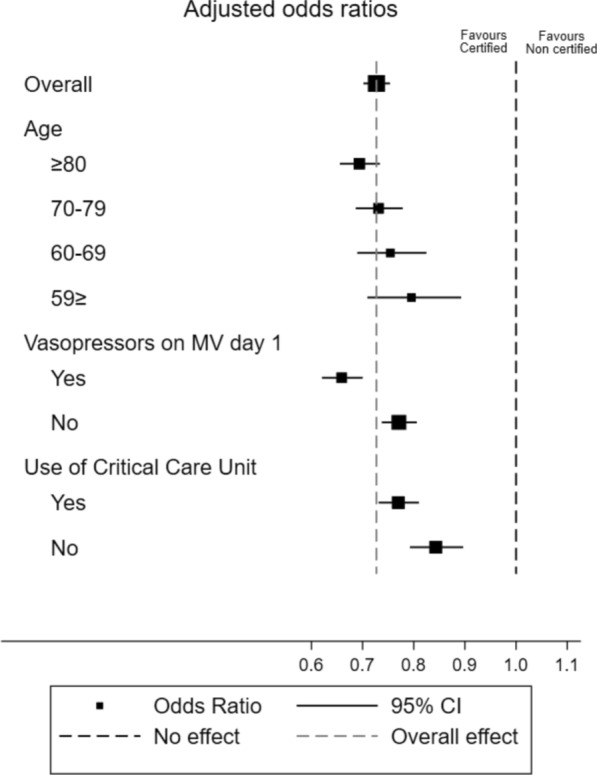
Results: Of the 66,905 patients in this study, 30,588 were treated at board-certified facilities, and 36,317 were not. The following differed between board-certified and non-certified facilities: propofol (35% vs. 18%), dexmedetomidine (37% vs. 19%), fentanyl (50% vs. 20%), rocuronium (8.5% vs. 2.6%), vecuronium (1.9% vs. 0.6%), noradrenaline (35% vs. 19%), arginine vasopressin (8.1% vs. 2.0%), adrenaline (2.3% vs. 1.0%), dobutamine (8.7% vs. 4.8%), phosphodiesterase inhibitors (1.0% vs. 0.3%), early enteral nutrition (29% vs. 14%), early rehabilitation (34% vs. 30%), renal replace therapy (15% vs. 6.7%), extracorporeal membrane oxygenation (1.6% vs. 0.3%), critical care unit admission (74% vs. 30%), dopamine (9.0% vs. 15%), sivelestat (4.1% vs. 7.0%), and high-dose methylprednisolone (13% vs. 15%). After 1:1 propensity score matching, the board-certified group had lower in-hospital mortality than the non-certified group (31% vs. 38%; odds ratio, 0.75; 95% confidence interval, 0.72-0.77; P < 0.001). Subgroup analyses showed greater benefits in the board-certified group for older patients, those who required vasopressors on the first day of mechanical ventilation, and those treated in critical care units.
Conclusions: Board-certified intensive care training facilities implemented several different adjunctive treatments for severe respiratory failure compared to non-board-certified facilities, and board-certified facilities were associated with lower in-hospital mortality. Because various factors may contribute to the outcome, the causal relationship remains uncertain. Further research is warranted to determine how best to strengthen patient outcomes in the critical care system through the certification of intensive care training facilities.
Keywords: Acute respiratory distress syndrome; Clinical practice; Intensivist; National in-patient database; Severe respiratory failure.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Ethics Committee of Yokohama City University approved this study (no. F220300054). Informed consent was not required because of the observational and anonymous nature of data collection. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
