

Sacubitril/valsartan preserves regional cardiac function following myocardial infarction in rats
- PMID: 39696842
- PMCID: PMC11911584
- DOI: 10.1002/ehf2.15145
Sacubitril/valsartan preserves regional cardiac function following myocardial infarction in rats
Abstract
Aims: Sacubitril/valsartan (Sac/Val) is used for treatment of heart failure. The effect of Sac/Val on regional dysfunction following myocardial infarction (MI) remains uncertain. This study aimed at understanding the effects of Sac/Val on regional function after MI.
Methods and results: MI or sham surgery was performed in Sprague-Dawley rats. Animals were randomized to treatment with Sac/Val, valsartan (Val) or vehicle (Veh). Magnetic resonance imaging was used to acquire left ventricular volumes and strain. Left ventricular tissue was obtained for wesern blotting, PCR and Masson's trichrome staining. Isolated cardiac fibroblasts were cultured with Veh, atrial natriuretic peptide (ANP), adrenomedullin (ADM) and sacubitrilat, and collagen expression assessed with droplet digital PCR.
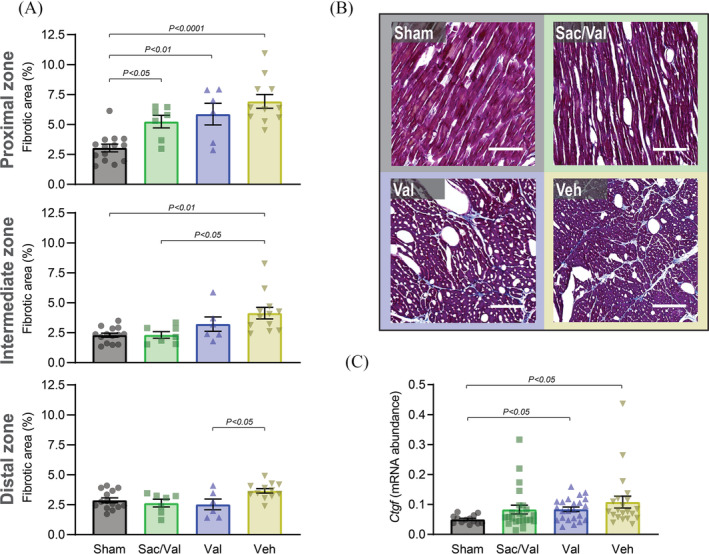
Results: Sac/Val reduced ventricular end-diastolic volume by 18% compared with Veh, and preserved circumferential systolic strain in the zone proximal to infarction compared with sham after 42 days of treatment (peak strain ± SEM: sham: -0.19 ± 0.01%; Sac/Val: -0.14 ± 0.02%; Val: -0.10 ± 0.02%; Veh: -0.10 ± 0.02%). Masson's trichrome staining demonstrated lower fibrotic deposition in the intermediate zone with Sac/Val treatment than Veh (sham: 2.29 ± 0.17%; Sac/Val: 2.31 ± 0.27%; Val: 3.22 ± 0.60%; Veh: 4.14 ± 0.48%). The amounts of the pro-apoptotic caspase 3 cleavage fragments p19/17 were 89% higher in Val than sham, with Sac/Val showing no significant increase compared with sham. Collagen expression in human fibroblast culture was lower in cells co-treated with sacubitrilat and ANP, an effect not observed with sacubitrilat/ADM co-treatment.
Conclusions: Sac/Val preserves in vivo myocardial function in the region most proximal to MI in rats and reduces left ventricular dilatation. These effects may be related to a reduction in both fibrosis and pro-apoptotic signalling.
Keywords: ARNi; Heart failure; Myocardial infarction; Regional function; Sacubitril/valsartan.
© 2024 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Sacubitril/valsartan and valsartan utilized for in vivo studies were received free of charge from Novartis AG. Dr. Hussain was an employee of Novartis AG at time of study conduct. The other authors declare that they do not have any conflict of interest.
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
