

Comparison of balloon catheter and oral misoprostol for cervical ripening in women with pre-labor rupture of membranes: A Finnish randomized controlled trial
- PMID: 39697073
- PMCID: PMC11782060
- DOI: 10.1111/aogs.15036
Comparison of balloon catheter and oral misoprostol for cervical ripening in women with pre-labor rupture of membranes: A Finnish randomized controlled trial
Abstract
Introduction: Pre-labor rupture of membranes (PROM) occurs in about 8% of term pregnancies with over 70% delivering spontaneously within 24 h. However, prolonged PROM increases the risk of chorioamnionitis and neonatal sepsis. While misoprostol and oxytocin are considered safe and effective methods of labor induction, most guidelines do not encourage balloon catheter (BC) use following PROM given concerns about increased risk of chorioamnionitis. However, lack of robust evidence exists. This study aimed to compare BC and low-dose oral misoprostol (OM) regarding infectious morbidity and assess the impact of routine antibiotic prophylaxis during BC use on infection prevention.
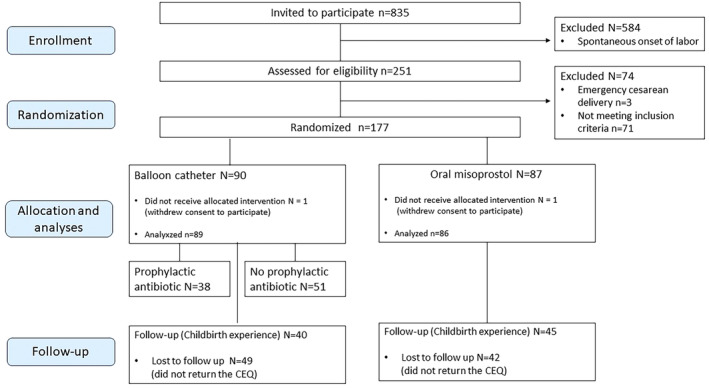
Material and methods: A randomized controlled trial comparing BC and low-dose 25 μg OM for pre-induction cervical ripening in an inpatient setting and assessing the preventive effect of prophylactic antibiotics during BC use in 175 women with PROM was carried out between 1.2.2021 and 31.12.2023 in Helsinki University Hospital. The study protocol was registered in the ISCTN registry (ISRCTN10972090). The primary outcome measures of the study were the mode of delivery, and maternal and neonatal infections.
Results: Eighty-nine women (50.9%) were allocated in the BC arm and 86 women (49.1%) in the OM arm. The cesarean delivery rates were comparable (BC 19.1% [n = 17] vs. OM 11.6% [n = 10]; p = 0.17). The rate of chorioamnionitis (BC 9.1% [n = 8] vs. OM 3.5% [n = 3]; p = 0.21) or neonatal infection (BC 4.5% [n = 4] vs. OM 2.3% [n = 2]; p = 0.68) were not statistically significantly different between the groups, although there was a trend towards higher frequency of infections in the BC arm. There were no differences in the incidence of chorioamnionitis or neonatal infections when routine antibiotic prophylaxis was administered during the BC use compared to those who did not receive antibiotics (chorioamnionitis 10.9% with antibiotics vs. 8.0% without antibiotics; p = 0.68, and neonatal infection 5.3% vs. 3.9%; p = 1.00). Maternal childbirth satisfaction was similar in the BC and OM groups.
Conclusions: Our results showed almost threefold frequency of chorioamnionitis and twofold frequency of neonatal infections following the use of BC compared to OM, although the study was underpowered for reaching statistical significance. The use of prophylactic antibiotics during BC retention did not reduce the incidence of infections.
Keywords: Oral misoprostol; balloon catheter; cervical ripening; chorioamnionitis; induction of labor; neonatal infection; pre‐labor rupture of membranes (PROM).
© 2024 The Author(s). Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hannah ME, Ohlsson A, Farine D, et al. Induction of labor compared with expectant management for prelabor rupture of the membranes at term. TERMPROM study group. N Engl J Med. 1996;18(334):1005‐1010. - PubMed
-
- Prelabor Rupture of Membranes . ACOG practice bulletin, number 217. Obstet Gynecol. 2020;135:e80‐e97. - PubMed
-
- Bellussi F, Melamed N, Barrett J, Berghella V. Term prelabor rupture of membranes: immediate induction is the optimal management. Am J Obstet Gynecol MFM. 2023;5:101094. - PubMed
-
- Bellussi F, Seidenari A, Juckett L, Di Mascio D, Berghella V. Induction within or after 12 hours of ≥36 weeks' prelabor rupture of membranes: a systematic review and meta‐analysis. Am J Obstet Gynecol MFM. 2021;3:100425. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
