

Multimodality Imaging in the Diagnosis and Staging of Gestational Choriocarcinoma
- PMID: 39697498
- PMCID: PMC11651844
- DOI: 10.1055/s-0044-1788590
Multimodality Imaging in the Diagnosis and Staging of Gestational Choriocarcinoma
Abstract
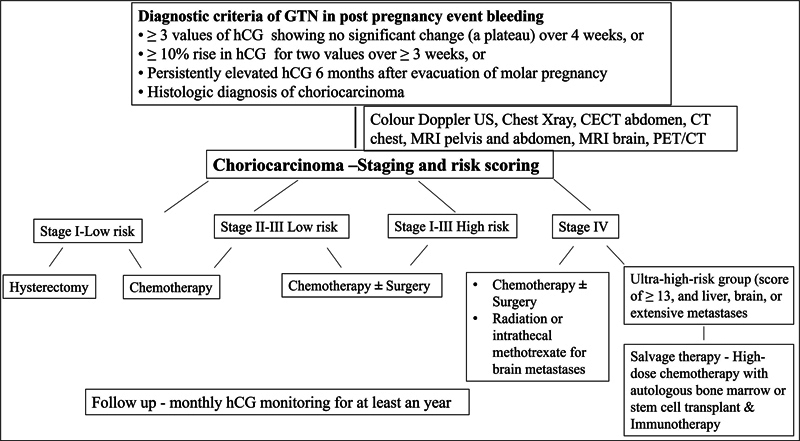
Choriocarcinoma is an uncommon, highly invasive malignancy arising from the placental trophoblastic tissue. Though staging is clinical, imaging has significant role in the diagnosis, staging, prognostic risk scoring, and management of choriocarcinomas. The purpose of this article is to review the role of multimodality imaging in the diagnosis, staging, and management of choriocarcinomas in correlation with clinicopathologic findings.
Keywords: choriocarcinoma; color Doppler; computed tomography; magnetic resonance imaging; positron emission tomography; ultrasound.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures


References
-
- Amin M B, Edge S, Greene F . 8th ed. Cham: Springer International Publishing; 2017. AJCC Cancer Staging Manual; pp. 257–260.
-
- Ngan H Y, Bender H, Benedet J L et al.FIGO Committee on Gynecologic Oncology. Gestational trophoblastic neoplasia, FIGO 2000 staging and classification. Int J Gynaecol Obstet. 2003;83:75–77. - PubMed
-
- Expert Panel on Women's Imaging Panel Dudiak K M, Maturen K E, Akin E Aet al.ACR appropriateness criteria® Gestational trophoblastic disease J Am Coll Radiol 201916(11S):S348–S363. - PubMed
-
- Ober W B, Fass R O. The early history of choriocarcinoma. J Hist Med Allied Sci. 1961;16:49–73. - PubMed
-
- Soper J T. Gestational trophoblastic disease. Obstet Gynecol. 2006;108(01):176–187. - PubMed
Publication types
LinkOut - more resources
Full Text Sources