

Sonographic Assessment of Isthmocele and Its Obstetric Complications in Subsequent Pregnancies: A Pictorial Review
- PMID: 39697515
- PMCID: PMC11651832
- DOI: 10.1055/s-0044-1788588
Sonographic Assessment of Isthmocele and Its Obstetric Complications in Subsequent Pregnancies: A Pictorial Review
Abstract
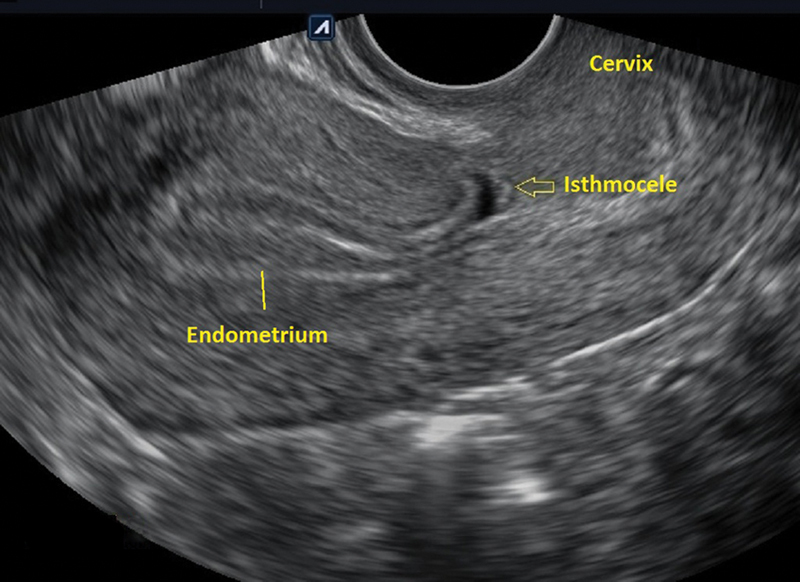
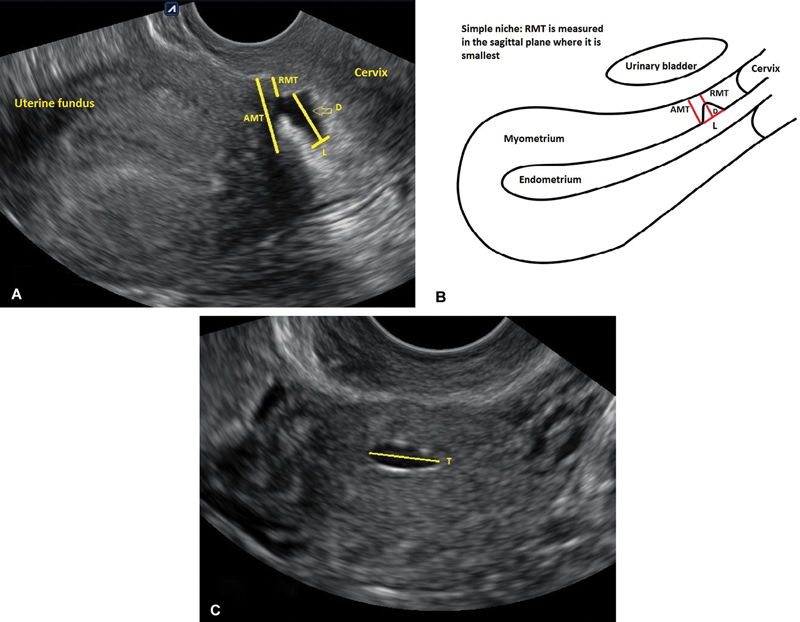
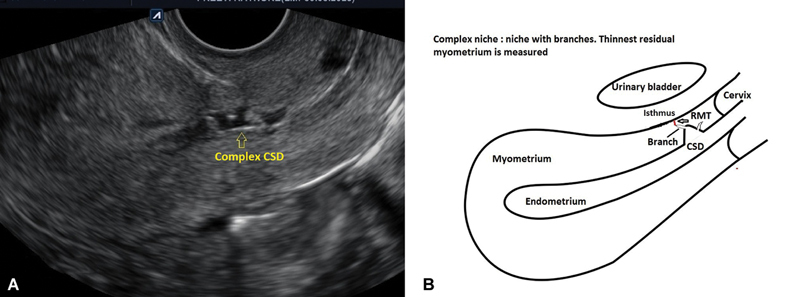
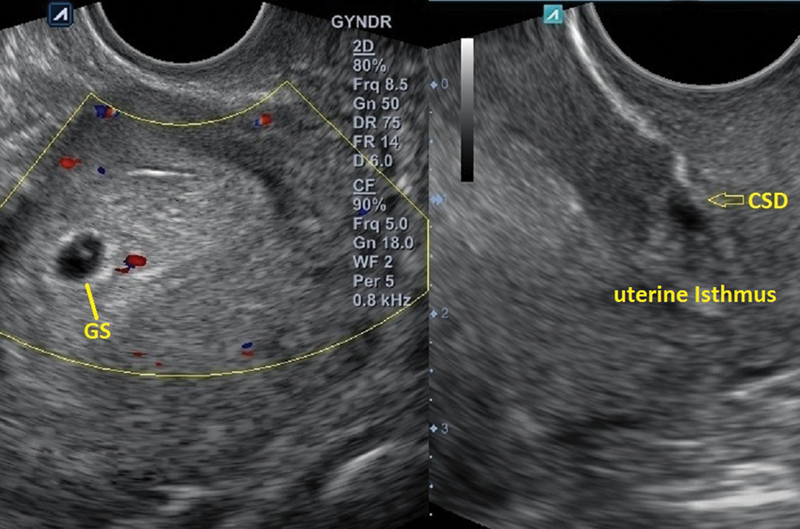
Cesarean scar defect represents a significant pathology attributed to the rising prevalence of cesarean deliveries. While not commonplace, these lesions can give rise to severe obstetric consequences during subsequent pregnancies. Given the potential complications, it is advisable to screen for uterine niches using transvaginal ultrasound (TVUS) or contrast-enhanced TVUS for individuals planning to conceive. Surgical repair and correction of these lesions can be crucial in averting obstetric and perinatal complications in future pregnancies. Furthermore, timely sonographic evaluation and reporting of isthmocele-related obstetric complications can help avoid serious issues.
Keywords: cesarean scar pregnancy; cesarean section; isthmocele; placenta accreta spectrum; retained products of conception; sonography.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures
Similar articles
-
Perinatal assessment of complex cesarean delivery: beyond placenta accreta spectrum.Am J Obstet Gynecol. 2023 Aug;229(2):129-139. doi: 10.1016/j.ajog.2023.02.021. Epub 2023 Mar 2. Am J Obstet Gynecol. 2023. PMID: 36868338
-
Diagnosis and management of isthmocele (Cesarean scar defect): a SWOT analysis.Ultrasound Obstet Gynecol. 2023 Sep;62(3):336-344. doi: 10.1002/uog.26171. Ultrasound Obstet Gynecol. 2023. PMID: 36730180 Review.
-
Comparison of transvaginal ultrasound and saline contrast sonohysterography in evaluation of cesarean scar defect: a prospective cohort study.Acta Obstet Gynecol Scand. 2018 Sep;97(9):1130-1136. doi: 10.1111/aogs.13367. Epub 2018 May 29. Acta Obstet Gynecol Scand. 2018. PMID: 29754409
-
Transvaginal Isthmocele Repair With Temporary Occlusion of Uterine Vessels in Caesarean Scar Pregnancy.Cureus. 2024 Feb 25;16(2):e54899. doi: 10.7759/cureus.54899. eCollection 2024 Feb. Cureus. 2024. PMID: 38544604 Free PMC article.
-
Reproductive outcomes following cesarean scar pregnancy - a case series and review of the literature.Eur J Obstet Gynecol Reprod Biol. 2016 May;200:102-7. doi: 10.1016/j.ejogrb.2016.02.039. Epub 2016 Mar 8. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 27014853 Review.
References
-
- van der Voet L F, Bij de Vaate A M, Veersema S, Brölmann H AM, Huirne J AF. Long-term complications of caesarean section. The niche in the scar: a prospective cohort study on niche prevalence and its relation to abnormal uterine bleeding. BJOG. 2014;121(02):236–244. - PubMed
-
- Bij de Vaate A J, Brölmann H AM, van der Voet L F, van der Slikke J W, Veersema S, Huirne J A. Ultrasound evaluation of the Cesarean scar: relation between a niche and postmenstrual spotting. Ultrasound Obstet Gynecol. 2011;37(01):93–99. - PubMed
-
- Glavind J, Madsen L D, Uldbjerg N, Dueholm M. Cesarean section scar measurements in non-pregnant women using three-dimensional ultrasound: a repeatability study. Eur J Obstet Gynecol Reprod Biol. 2016;201:65–69. - PubMed
-
- Fiocchi F, Petrella E, Nocetti L et al.Transvaginal ultrasound assessment of uterine scar after previous caesarean section: comparison with 3T-magnetic resonance diffusion tensor imaging. Radiol Med (Torino) 2015;120(02):228–238. - PubMed
-
- van der Voet L LF, Limperg T, Veersema S et al.Niches after cesarean section in a population seeking hysteroscopic sterilization. Eur J Obstet Gynecol Reprod Biol. 2017;214:104–108. - PubMed
LinkOut - more resources
Full Text Sources