

Metastatic papillary thyroid carcinoma in the soft tissue of the breast in a male patient: A case report
- PMID: 39697978
- PMCID: PMC11653250
- DOI: 10.3892/ol.2024.14841
Metastatic papillary thyroid carcinoma in the soft tissue of the breast in a male patient: A case report
Abstract
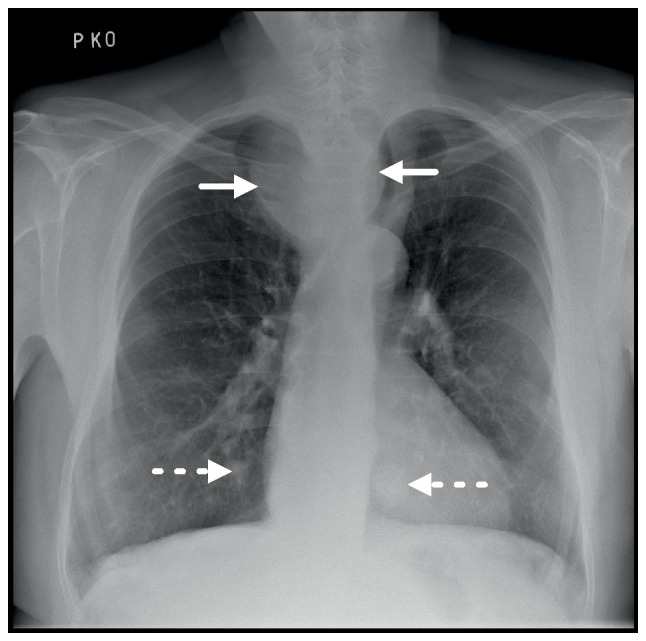
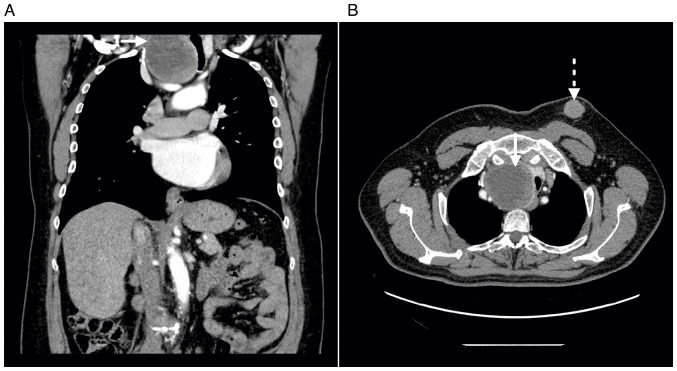
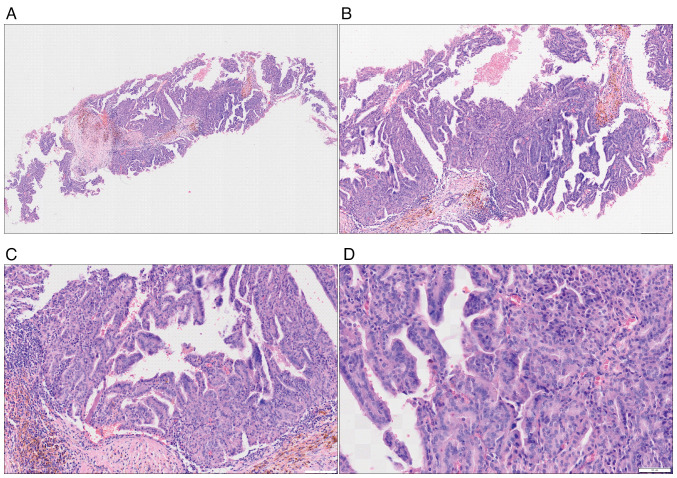
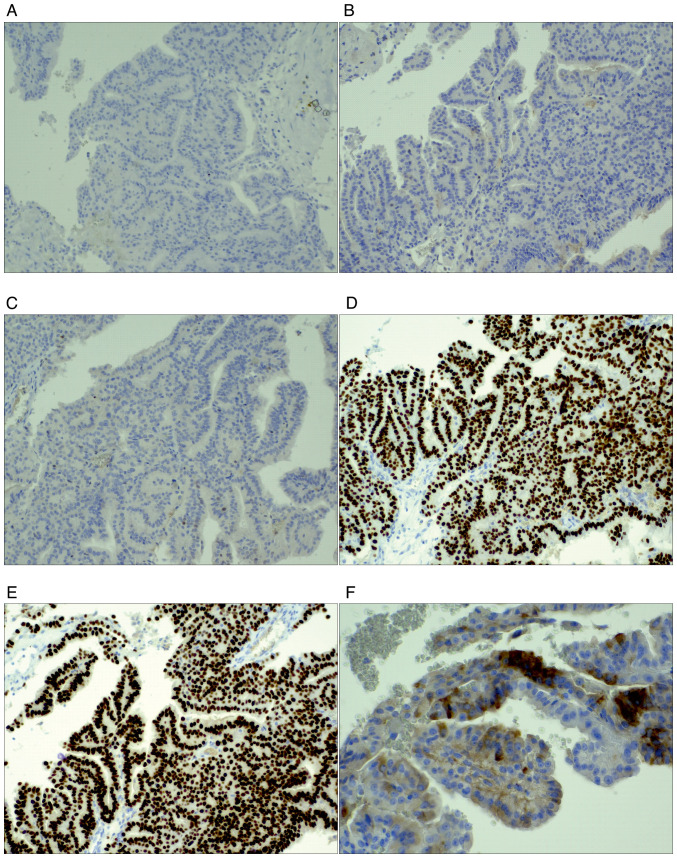
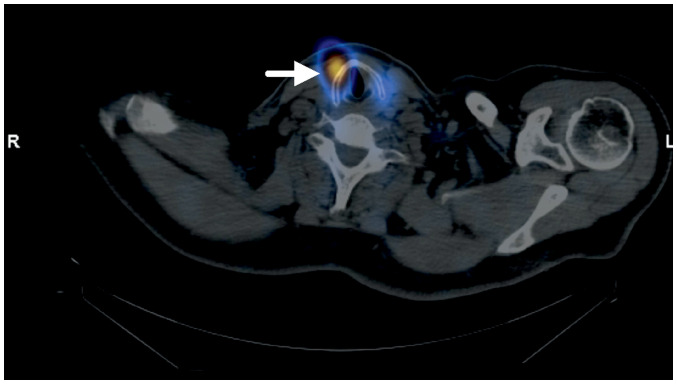
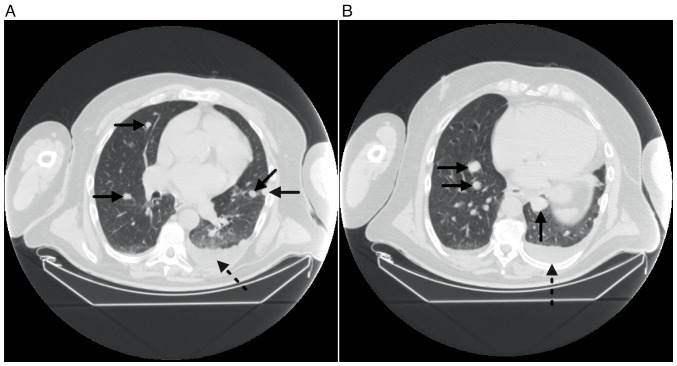
Papillary thyroid carcinoma (PTC) represents ~80% of all thyroid cancers, most frequently presenting in women in the third and fourth decade of life. The first clinical manifestation of PTC commonly includes a palpable mass in the thyroid area or cervical lymphadenopathy in cases of metastatic disease. Hematogenous distant metastases are a sign of an advanced stage of the tumour. The present study reported an extremely rare occurrence of solitary metastasis of a PTC in the left breast of a 63-year-old male patient, mimicking primary male breast cancer (MBC). The presence of a male breast lesion that did not follow the typical imaging criteria for MBC aroused suspicion of a different primary origin. The combination of imaging methods, laboratory findings and fine-needle aspiration techniques enabling cytological and histopathological examination, with the use of a wide panel of immunohistochemical markers, is crucial to establishing a definitive and correct diagnosis.
Keywords: PTC; breast metastasis; mediastinal mass; soft-tissue metastasis.
Copyright: © 2024 Maráčková et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Podolski A, Castelluci E, Halmos B. Precision medicine: BRAF mutations in thyroid cancer. Precis Cancer Med. 2019;2:29. doi: 10.21037/pcm.2019.09.04. - DOI
Publication types
LinkOut - more resources
Full Text Sources