

Does Chronic Kidney Disease Influence Revascularization Strategy After Acute Coronary Syndrome? A Systematic Review and Meta-Analysis
- PMID: 39698011
- PMCID: PMC11650572
- DOI: 10.14740/cr1731
Does Chronic Kidney Disease Influence Revascularization Strategy After Acute Coronary Syndrome? A Systematic Review and Meta-Analysis
Abstract
Background: Coronary artery bypass grafting (CABG) provides superior long-term outcomes to percutaneous coronary intervention (PCI) for complex multivessel coronary artery disease (CAD). People with chronic kidney disease (CKD) have increased prevalence of multivessel CAD, but also increased surgical risk. We investigated whether CKD predicted real-world use of CABG, versus PCI, in patients revascularized for acute coronary syndrome (ACS).
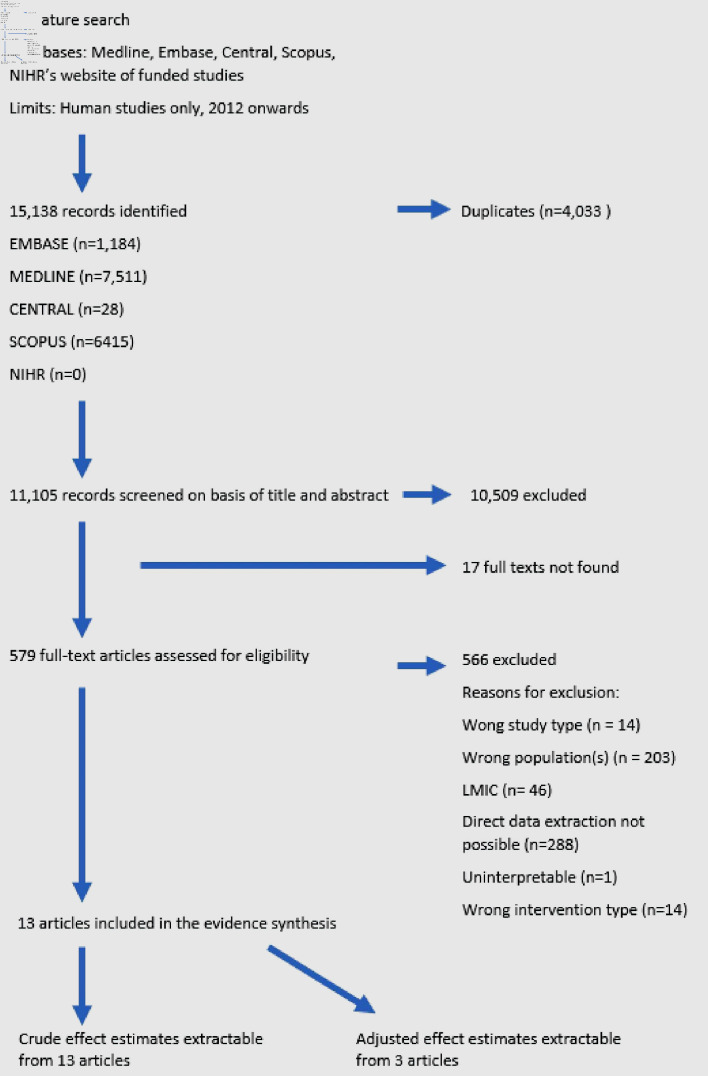
Methods: Embase, MEDLINE, Scopus and CENTRAL were searched to identify articles referring to ACS and invasive coronary intervention in high-income countries (2012 - 2023). Articles were included if CABG rates were reported in ACS patients with and without CKD receiving revascularization. CKD was defined as an estimated glomerular filtration rate < 60 mL/min/1.73 m2; proxy definitions were accepted. Random effect meta-analyses were used to determine the average effect of CKD on odds of CABG, stratified by ACS type and dialysis use.
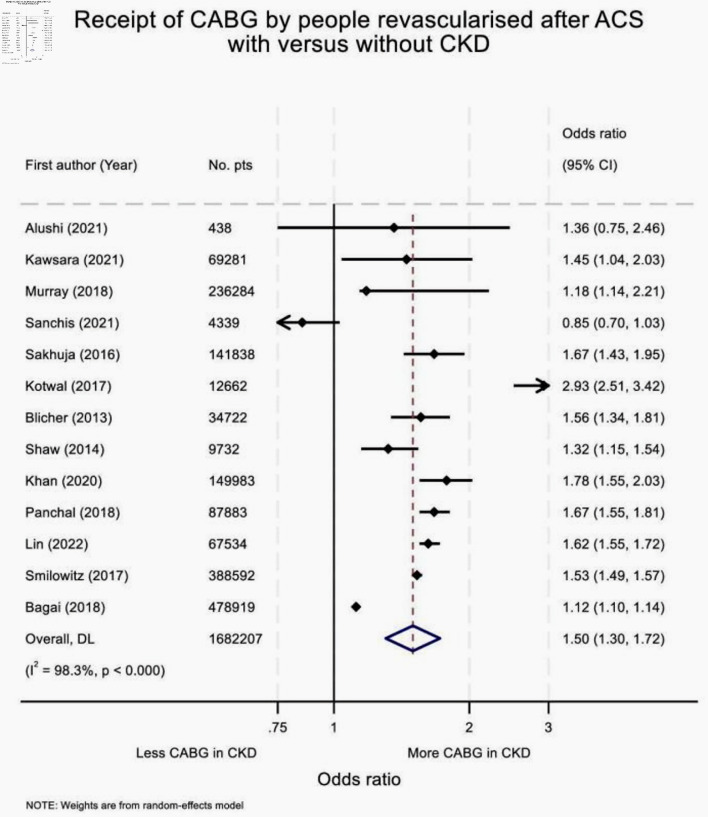
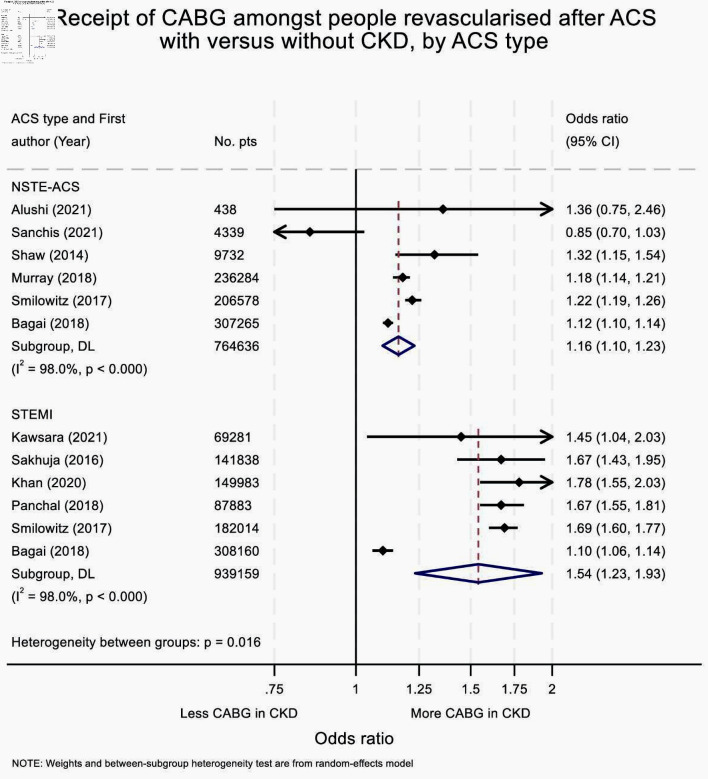
Results: Searches generated 15,138 articles, of which 13 observational studies were included (n = 1,682,207). Amongst revascularized ACS patients, those with CKD were more likely to receive CABG than those without (pooled odds ratio (OR) = 1.50 (95% confidence interval (CI) = 1.30 - 1.72). This association was stronger following ST-elevation myocardial infarction (STEMI) than non-ST-elevation ACS (NSTE-ACS) (OR: 1.54 (95% CI: 1.23 - 1.93)) versus 1.16 (1.10 - 1.23), respectively).
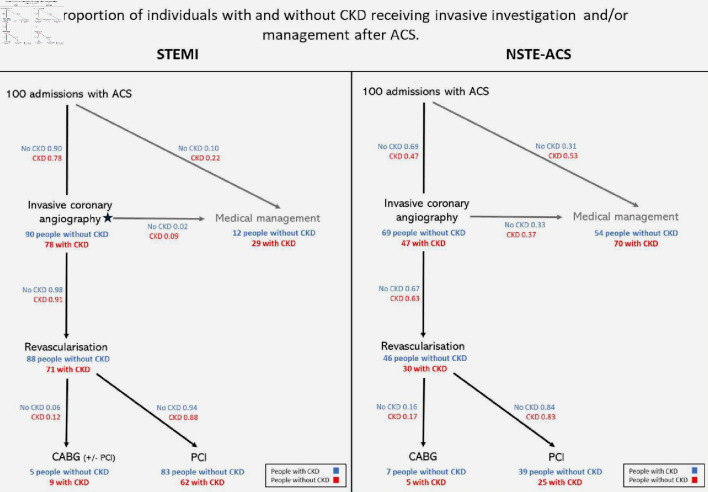
Conclusions: In high-income countries, revascularized ACS patients with CKD receive CABG (versus PCI) more frequently than those without kidney disease. However, accounting for lower use of coronary angiography in the CKD population removed this association following NSTE-ACS. Greater use of invasive angiography in those with NSTE-ACS and CKD might therefore increase access to revascularization, and thereby improve outcomes.
Keywords: Chronic kidney disease; Meta-analysis; Revascularization.
Copyright 2024, Scott et al.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Bhatia S, Arora S, Bhatia SM, Al-Hijji M, Reddy YNV, Patel P, Rihal CS. et al. Non-ST-segment-elevation myocardial infarction among patients with chronic kidney disease: a propensity score-matched comparison of percutaneous coronary intervention versus conservative management. J Am Heart Assoc. 2018;7(6) doi: 10.1161/JAHA.117.007920. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous