

Projecting the Population Level Burden of CKD Progression According to Urine Albumin-to-Creatinine Ratio Categories
- PMID: 39698359
- PMCID: PMC11652095
- DOI: 10.1016/j.ekir.2024.09.021
Projecting the Population Level Burden of CKD Progression According to Urine Albumin-to-Creatinine Ratio Categories
Abstract
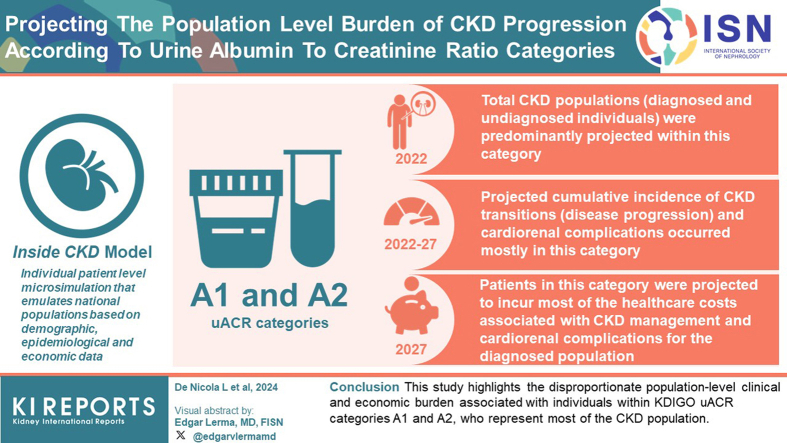
Introduction: Urinary albumin-to-creatinine ratio (uACR) is an independent predictor of chronic kidney disease (CKD) progression. However there is limited evidence on the burden of CKD according to uACR categories at the population level. This study estimates future clinical and financial burden of CKD according to uACR categories using the Inside CKD microsimulation.
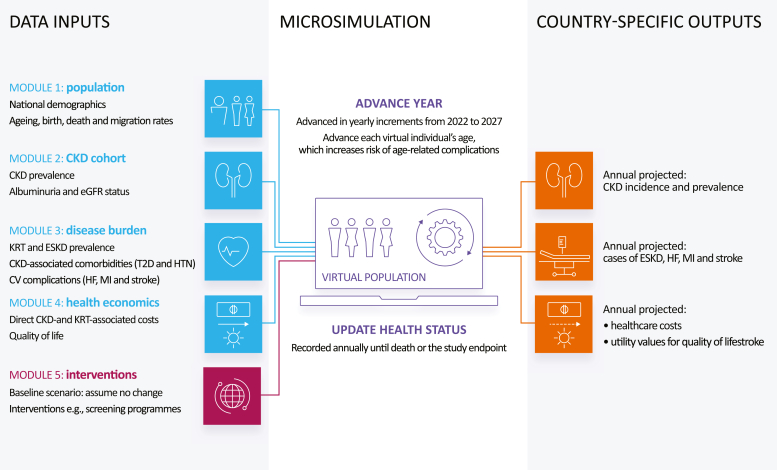
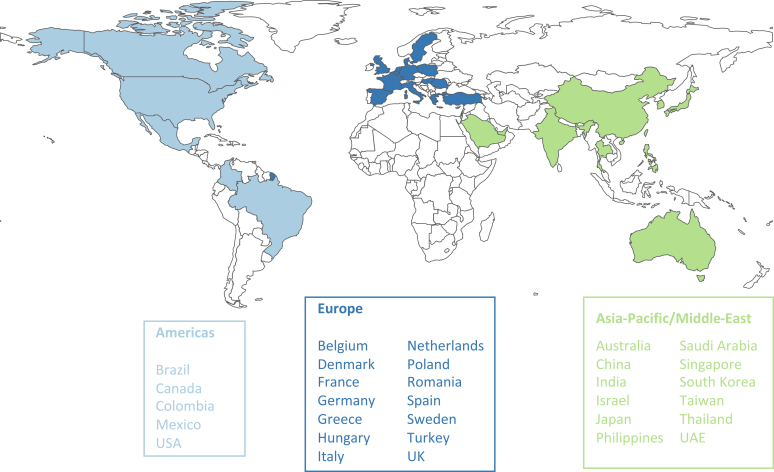
Methods: The Inside CKD model is an individual patient level microsimulation that emulates national populations based on demographic, epidemiological, and economic data. The analysis estimates clinical and economic outcomes over time according to the Kidney Disease: Improving Global Outcomes (KDIGO) uACR categories (A1-A3) at a population level for 31 countries and regions.
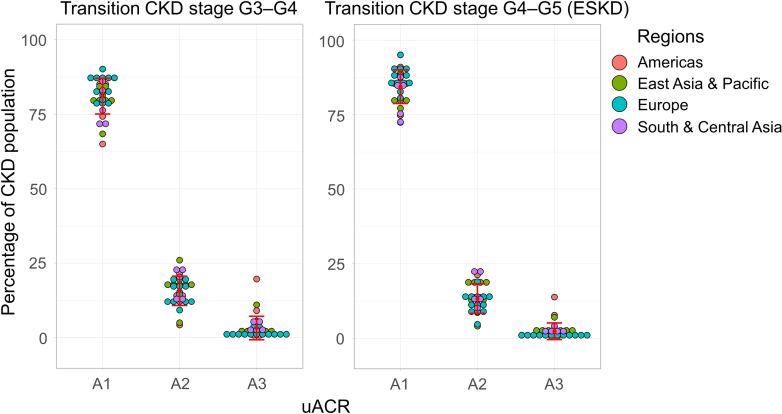
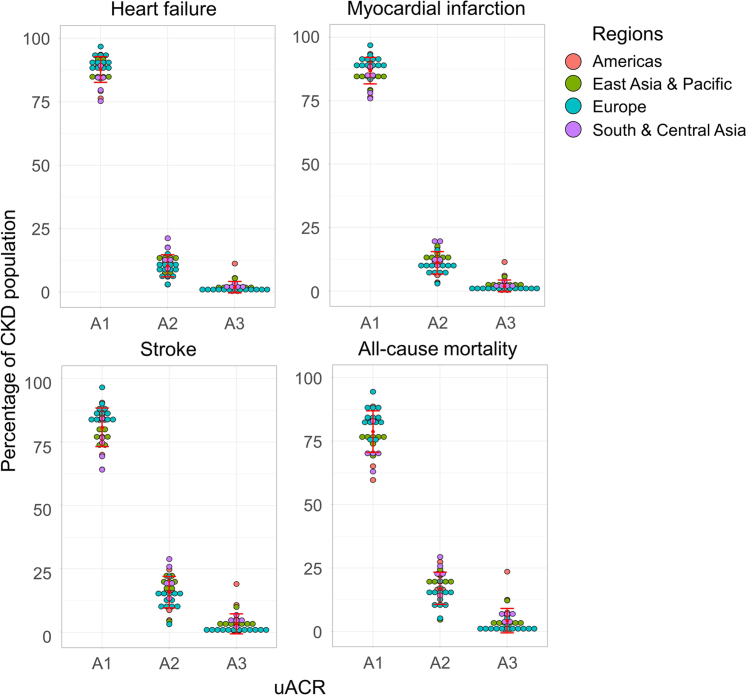
Results: CKD populations (diagnosed and undiagnosed individuals, stages G3-G5) were projected to be predominantly within uACR categories A1 and A2 in 2022. Projected cumulative incidence of CKD stage transitions (disease progression) and cardio-renal complications (heart failure, myocardial infarction, stroke, and all-cause mortality) occurred mostly in uACR categories A1 and A2 between 2022 and 2027. Patients in uACR categories A1 and A2, who represent the largest proportion of patients with CKD, were projected to incur most of the health care costs associated with CKD management and cardio-renal complications for the diagnosed population (prevalence 2027).
Conclusion: This study highlights the disproportionate population-level clinical and economic burden associated with individuals within KDIGO uACR categories A1 and A2, who represent most of the CKD population. This awareness will help health care decision makers to appropriately allocate resources and interventions to the CKD population, including those with mild to moderately increased albuminuria, to reduce clinical and economic burden associated with CKD.
Keywords: burden of disease; cardio-renal complication; chronic kidney disease; economic burden; end-stage kidney disease; urine albumin-to-creatinine ratio.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Shlipak M.G., Tummalapalli S.L., Boulware L.E., et al. The case for early identification and intervention of chronic kidney disease: conclusions from a Kidney Disease: improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2021;99:34–47. doi: 10.1016/j.kint.2020.10.012. - DOI - PubMed
-
- Foreman K.J., Marquez N., Dolgert A., et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392:2052–2090. doi: 10.1016/S0140-6736(18)31694-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
