

Long-Term Outcome of Childhood Asthma: Characterizing COPD-A and COPD-C Subtypes in Adulthood
- PMID: 39698488
- PMCID: PMC11653850
- DOI: 10.2147/JAA.S474417
Long-Term Outcome of Childhood Asthma: Characterizing COPD-A and COPD-C Subtypes in Adulthood
Abstract
Background and aim: Asthma in early life has been linked to subsequent development of COPD and according to GOLD 2023 COPD may be divided into distinct subtypes. We aimed to investigate factors associated with the GOLD classification COPD-A (asthma in childhood) and COPD-C (tobacco exposure) in a cohort of adults with a history of severe childhood asthma.
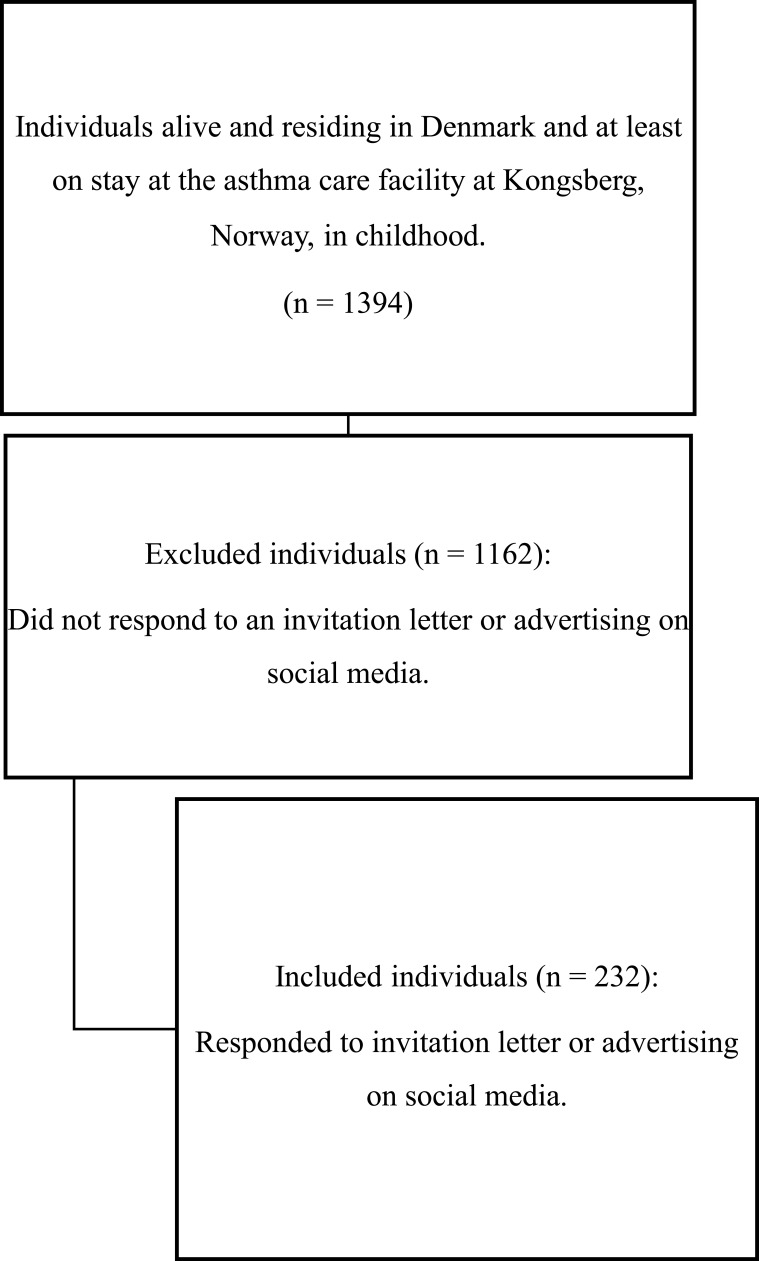
Patients and methods: In a cohort of Danish adults with a history of severe childhood asthma and a previous 4-month stay during childhood at the asthma care facility in Kongsberg, Norway, we divided participants in a long-term follow-up examination into COPD-A and COPD-C, defined as post-bronchodilator FEV1/FVC < 0.7, and never-smoker or ever-smoker, respectively, and no airflow limitation. Characteristics between groups were analysed.
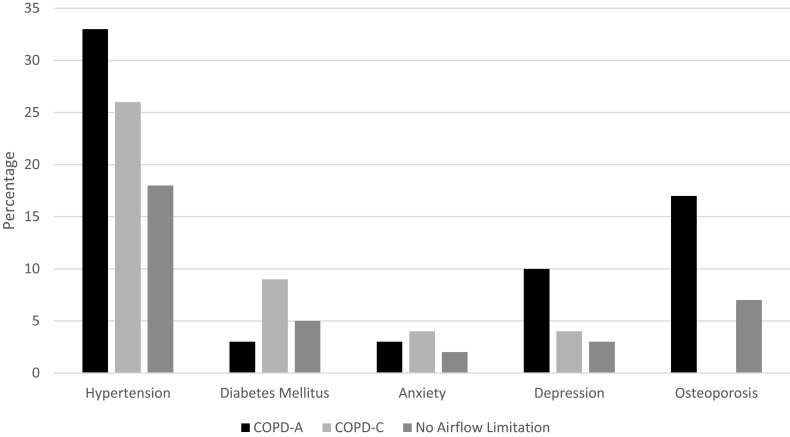
Results: The study cohort comprised 232 adults with a history of severe childhood asthma, of whom 30 (13%) and 23 (10%), respectively, were classified as COPD-A and COPD-C. Compared to those with no airflow limitation, individuals with COPD-A and COPD-C more often had had at least one exacerbation (filled prescription of oral corticosteroid) in the past 12 months (risk ratio [RR] 1.83 and 2.65, respectively). The COPD-C group had a significantly higher Medical Research Council dyspnoea score (p<0.01) and significantly higher blood eosinophil count (p<0.01) than those with no airflow limitation. Compared to the COPD-C group, the COPD-A group had higher fractional exhaled nitric oxide (mean 29 [SD 28]) and FEV1%pred (mean 75 [SD 20]). Finally, when comparing participants with COPD-A to both COPD-C and participants without airflow limitation, the proportion of participants with osteoporosis (17%) and depression (10%) was more than twice as high.
Conclusion: Our study revealed a high prevalence and unique features of the two COPD subtypes COPD-A and COPD-C in a cohort of adults with a history of severe childhood asthma.
Keywords: Kongsberg cohort; adult; asthma; early life; etiotypes.
© 2024 Savran et al.
Conflict of interest statement
The authors report no conflicts of interest related to the paper. Outside the submitted work, OS has received personal fees for advisory board meeting from GSK. CSU has received grants, consulting fees, speaker’s fees and fees for attending advisory boards etc. from Sanofi, Boehringer Ingelheim, AstraZeneca, Novartis, Covis Pharma, Novo Nordisk, Chiesi, Orion Pharma, Takeda, Roche, GSK, TEVA, Berlin Chemie, Hikma Pharmaceuticals, TFF Pharmaceuticals, Actelion, and Pfizer.
Figures
References
-
- Global Initiative for Asthma. Global strategy for asthma management and prevention, 2023. Available from: www.ginaasthma.org. Accessed June 17, 2023.
-
- Global strategy for the diagnosis, management and prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 report. Available from: https://goldcopd.org/. Accessed June 17, 2023.
LinkOut - more resources
Full Text Sources
Miscellaneous
