

Exploring the optimal threshold of 3D consolidation tumor ratio value segmentation based on artificial intelligence for predicting the invasive degree of T1 lung adenocarcinoma
- PMID: 39698672
- PMCID: PMC11651987
- DOI: 10.21037/qims-24-1328
Exploring the optimal threshold of 3D consolidation tumor ratio value segmentation based on artificial intelligence for predicting the invasive degree of T1 lung adenocarcinoma
Abstract
Background: The assessment of lung adenocarcinoma significantly depends on the proportion of solid components in lung nodules. Traditional one-dimensional consolidation tumor ratio (1D CTR) based on ideal, uniformly dense solid components lacks precision. There is no consensus on the CT threshold for evaluating invasiveness using the threshold segmentation method. This study aimed to explore the effectiveness of the three-dimensional CTR (3D CTR) calculated by the artificial intelligence threshold segmentation method in predicting invasive stage T1 lung adenocarcinoma and to identify its optimal threshold and cut-off point.
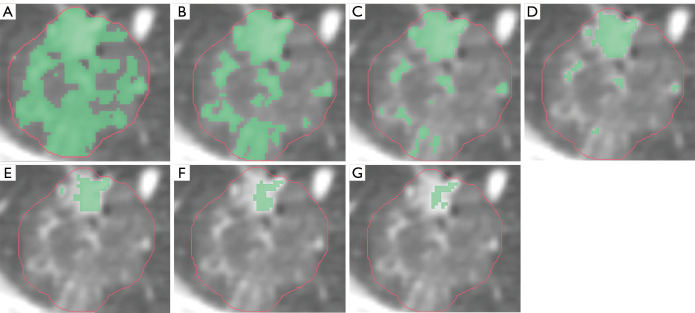
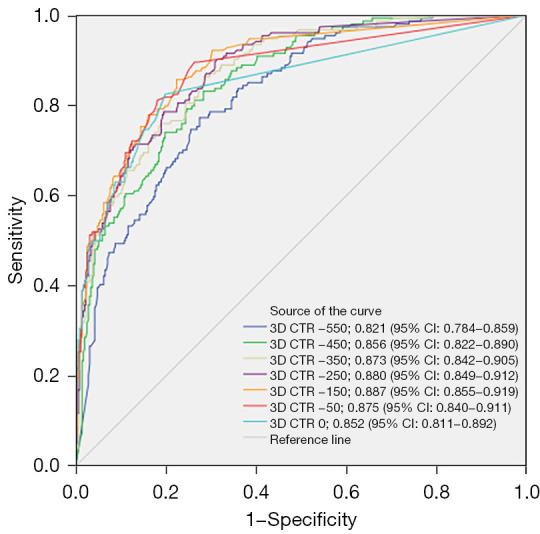
Methods: Data from 1,056 patients with 1,179 pulmonary nodules confirmed by postoperative pathology were collected retrospectively from two centers, Zhengzhou People's Hospital and Huadong Hospital of Fudan University. Patients were divided into non-invasive [atypical adenomatous hyperplasia (AAH), adenocarcinoma in situ (AIS), minimally invasive adenocarcinoma (MIA)] and invasive groups [invasive adenocarcinoma (IAC)]. Seven computed tomography (CT) threshold settings (-550 to 0 HU) were used to calculate the 3D CTR via the threshold segmentation method, and differences between the groups were analyzed. Receiver operating characteristic (ROC) curves were plotted to compare predictive performance for invasiveness of stage T1 lung adenocarcinoma, and the optimal threshold and corresponding cut-off value were determined. Subgroup analyses based on nodule size-T1a (≤10 mm), T1b (>10 to 20 mm), and T1c (>20 to 30 mm)-were also conducted.
Results: The CT threshold of -150 Housefield unit (HU) showed the highest predictive efficacy for invasiveness of stage T1 lung adenocarcinoma, with an area under the curve (AUC) of 0.901 [95% confidence interval (CI): 0.883-0.919], sensitivity of 86.878%, and specificity of 77.883%. The optimal cut-off point for 3D CTR was 2.75%. In subgroup analyses, -150 HU remained optimal, with predictive performance increasing with nodule size. For the T1a group, the AUC was 0.887 (95% CI: 0.885-0.919), cut-off value was 2.75%, sensitivity was 77.620%, and specificity was 85.714%. For the T1b group, values were 0.903 (95% CI: 0.875-0.931), cut-off value was 5.4%, sensitivity was 87.671%, and specificity was 80.296%. For the T1c group, values were 0.928 (95% CI: 0.893-0.963), cut-off value was 7.1%, sensitivity was 88.043%, and specificity was 81.176%.
Conclusions: This study suggests that setting the CT threshold at -150 HU and using the AI-based threshold segmentation method to calculate the 3D CTR effectively distinguishes whether stage T1 lung adenocarcinoma is invasive, with an optimal cut-off point at 2.75%. Under this threshold, for varying nodule sizes, criteria are proposed: for nodules ≤10 mm with a 3D CTR <2.75%; >10 to 20 mm with a 3D CTR <5.4%; and >20 to 30 mm with a 3D CTR <7.1%, these partially solid nodules can be treated as non-IAC.
Keywords: Artificial intelligence (AI); T1 stage lung adenocarcinoma; invasive adenocarcinoma (IAC); three-dimensional consolidation tumor ratio (3D CTR); threshold segmentation method.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-24-1328/coif). L.Z. is an employee of Shukun (Beijing) Technology Co. The other authors have no conflicts of interest to declare.
Figures





References
-
- Suzuki K, Koike T, Asakawa T, Kusumoto M, Asamura H, Nagai K, Tada H, Mitsudomi T, Tsuboi M, Shibata T, Fukuda H, Kato H, Japan Lung Cancer Surgical Study Group (JCOG LCSSG). A prospective radiological study of thin-section computed tomography to predict pathological noninvasiveness in peripheral clinical IA lung cancer (Japan Clinical Oncology Group 0201). J Thorac Oncol 2011;6:751-6. 10.1097/JTO.0b013e31821038ab - DOI - PubMed
-
- Suzuki K, Watanabe SI, Wakabayashi M, Saji H, Aokage K, Moriya Y, Yoshino I, Tsuboi M, Nakamura S, Nakamura K, Mitsudomi T, Asamura H, West Japan Oncology Group and Japan Clinical Oncology Group . A single-arm study of sublobar resection for ground-glass opacity dominant peripheral lung cancer. J Thorac Cardiovasc Surg 2022;163:289-301.e2. 10.1016/j.jtcvs.2020.09.146 - DOI - PubMed
-
- Saji H, Okada M, Tsuboi M, Nakajima R, Suzuki K, Aokage K, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet 2022;399:1607-17. 10.1016/S0140-6736(21)02333-3 - DOI - PubMed
-
- Aokage K, Suzuki K, Saji H, Wakabayashi M, Kataoka T, Sekino Y, et al. Segmentectomy for ground-glass-dominant lung cancer with a tumour diameter of 3 cm or less including ground-glass opacity (JCOG1211): a multicentre, single-arm, confirmatory, phase 3 trial. Lancet Respir Med 2023;11:540-9. 10.1016/S2213-2600(23)00041-3 - DOI - PubMed
LinkOut - more resources
Full Text Sources