

Gadoxetic acid disodium (Gd-EOB-DTPA) contrast-enhanced abbreviated magnetic resonance imaging (MRI) for hepatocellular carcinoma surveillance in at-risk patients: a multi-center study in China
- PMID: 39698720
- PMCID: PMC11651963
- DOI: 10.21037/qims-24-941
Gadoxetic acid disodium (Gd-EOB-DTPA) contrast-enhanced abbreviated magnetic resonance imaging (MRI) for hepatocellular carcinoma surveillance in at-risk patients: a multi-center study in China
Abstract
Background: Given the limited capacity and suboptimal sensitivity of ultrasonography (US), gadoxetic acid disodium (Gd-EOB-DTPA)-enhanced magnetic resonance imaging (MRI) demonstrates good diagnostic performance for hepatocellular carcinoma (HCC). Some researchers have proposed that the abbreviated MRI (AMRI) protocols have potential as a surveillance tool. However, few studies have compared multiple AMRI protocols with complete Gd-EOB-DTPA contrast-enhanced MRI for HCC surveillance. We aimed to explore and compare the diagnostic performance of 3 AMRI protocols as HCC surveillance in high-risk patients.
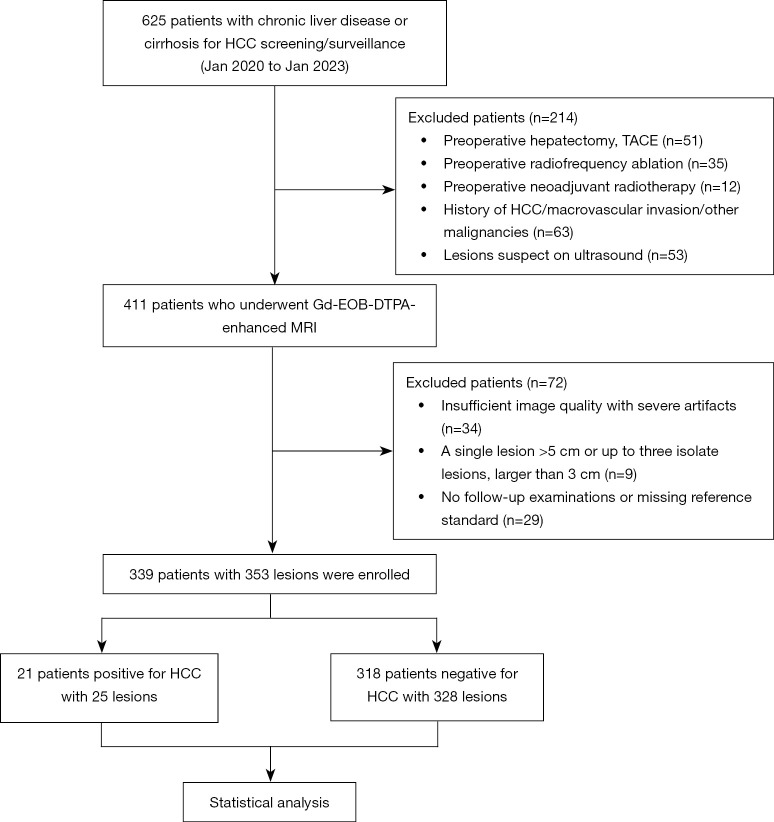
Methods: This multi-center, retrospective, blinded reader study conducted in China consecutively enrolled 339 patients with hepatitis and/or cirrhosis who underwent complete Gd-EOB-DTPA contrast-enhanced MRI for HCC surveillance from 2020 to 2023. We extracted 3 additional AMRI protocols: noncontrast-AMRI [NC-AMRI: T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI)]; dynamic-AMRI (Dyn-AMRI: early and late arterial phases, portal venous phase, and DWI); and hepatobiliary phase-AMRI (HBP-AMRI: T2WI, DWI, and HBP). Then, 2 independent radiologists assessed the AMRI and complete Gd-EOB-DTPA contrast-enhanced MRI protocols. Patients were classified as HCC positive/HCC negative based on the reference standard. Agreement was assessed using Kappa statistics. The acquisition time differences of the 4 MRI protocols were analyzed by analysis of variance (ANOVA). Per-lesion HCC diagnostic performances were compared by Cochran's Q test. Receiver operating characteristic (ROC) curves for the 3 AMRI protocols were evaluated, and the area under the ROC curve (AUROC) was calculated and compared by DeLong's test.
Results: A total of 353 lesions were detected in the 339 included patients, and 21/339 patients were diagnosed with HCC (prevalence, 6.2%). The inter-observer agreement was good for all 4 MRI protocols (k>0.75). Acquisition times differed significantly (P<0.001), from the shortest to the longest: NC-AMRI (263.44±5.05 s) < HBP-AMRI (269.18±4.93 s) < Dyn-AMRI (307.71±4.93 s) < complete Gd-EOB-DTPA contrast-enhanced MRI (582.03±3.59 s). The sensitivity (Cochran's Q=14.667, P=0.002) and specificity (Cochran's Q=59.682, P<0.001) of 4 MRI protocols were statistically significant. HBP-AMRI showed the highest sensitivity (84.00%), whereas Dyn-AMRI exhibited the highest specificity (99.39%) among 3 AMRI protocols. The per-lesion positive predictive value (PPV) for the NC-AMRI, Dyn-AMRI, and HBP-AMRI was 41.66%, 88.89%, and 47.72%, the corresponding negative predictive value (NPV) was 96.21%, 97.31%, and 98.70%, and the number needed to diagnose (NND) for the NC-AMRI, Dyn-AMRI, HBP-AMRI, and complete Gd-EOB-DTPA contrast-enhanced MRI was: 1.865, 1.577, 1.234, and 1.569, respectively. DeLong's test showed the AUROC value of either Dyn-AMRI or HBP-AMRI was significantly higher than that of NC-AMRI (Z=2.330, P=0.019; Z=2.680, P=0.007, respectively), but no significant difference between HBP-AMRI and Dyn-AMRI (Z=1.643, P=0.100).
Conclusions: AMRI protocols can be implemented in clinical practice as a patient-centered and tailored regimen for HCC surveillance in China. NC-AMRI might become an optional tool due to its minimal scanning time, lower cost, and exemption from contrast agents. Dyn-AMRI, achieving the highest specificity, is a reliable surveillance strategy. HBP-AMRI as a favorable alternative showed a high sensitivity and NPV while maintaining considerable specificity and NND.
Keywords: Hepatocellular carcinoma (HCC); abbreviated magnetic resonance imaging (AMRI); gadoxetic acid disodium (Gd-EOB-DTPA); surveillance.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-24-941/coif). The authors have no conflicts of interest to declare.
Figures




Similar articles
-
Gadoxetate-enhanced abbreviated MRI is highly accurate for hepatocellular carcinoma screening.Eur Radiol. 2020 Nov;30(11):6003-6013. doi: 10.1007/s00330-020-07014-1. Epub 2020 Jun 25. Eur Radiol. 2020. PMID: 32588209
-
The combination of non-contrast abbreviated MRI and alpha foetoprotein has high performance for hepatocellular carcinoma screening.Eur Radiol. 2023 Oct;33(10):6929-6938. doi: 10.1007/s00330-023-09906-4. Epub 2023 Jul 18. Eur Radiol. 2023. PMID: 37464111 Free PMC article.
-
Comparison of noncontrast, dynamic, and hepatobiliary phase abbreviated MRI protocols for detection of hepatic malignancies.Clin Imaging. 2023 Sep;101:206-214. doi: 10.1016/j.clinimag.2023.05.018. Epub 2023 Jun 12. Clin Imaging. 2023. PMID: 37421716
-
Gadoxetic acid disodium-enhanced magnetic resonance imaging outperformed multidetector computed tomography in diagnosing small hepatocellular carcinoma: A meta-analysis.Liver Transpl. 2017 Dec;23(12):1505-1518. doi: 10.1002/lt.24867. Liver Transpl. 2017. PMID: 28886231
-
Meta-Analysis of the Accuracy of Abbreviated Magnetic Resonance Imaging for Hepatocellular Carcinoma Surveillance: Non-Contrast versus Hepatobiliary Phase-Abbreviated Magnetic Resonance Imaging.Cancers (Basel). 2021 Jun 14;13(12):2975. doi: 10.3390/cancers13122975. Cancers (Basel). 2021. PMID: 34198589 Free PMC article. Review.
References
-
- Yokoo T, Masaki N, Parikh ND, Lane BF, Feng Z, Mendiratta-Lala M, Lee CH, Khatri G, Marsh TL, Shetty K, Dunn CT, Al-Jarrah T, Aslam A, Davenport MS, Gopal P, Rich NE, Lok AS, Singal AG. Multicenter Validation of Abbreviated MRI for Detecting Early-Stage Hepatocellular Carcinoma. Radiology 2023;307:e220917. 10.1148/radiol.220917 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous