

Diagnostic Efficacy of 11 SARS-CoV-2 Serological Assays for COVID-19: A Meta-Analysis and Adjusted Indirect Comparison of Diagnostic Test Accuracy
- PMID: 39698931
- PMCID: PMC11656407
- DOI: 10.1002/iid3.70114
Diagnostic Efficacy of 11 SARS-CoV-2 Serological Assays for COVID-19: A Meta-Analysis and Adjusted Indirect Comparison of Diagnostic Test Accuracy
Abstract
Objective: In the past 5 years, a large number of serological assays for large-scale detection of antibodies against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigen emerged. Serological assays for SARS-CoV-2 were needed to support clinical diagnosis and epidemiological investigations. However, there were limited data on the diagnostic accuracy of these serological assays. We aimed to compare the diagnostic accuracy of 11 commercial serological assays for coronavirus disease-2019 (COVID-19) by taking the reverse transcriptase polymerase chain reaction (RT-PCR) assays as the reference standard, which served as the control arm to conduct an indirect comparison of diagnostic accuracy for 11 different SARS-CoV-2 serological assays.
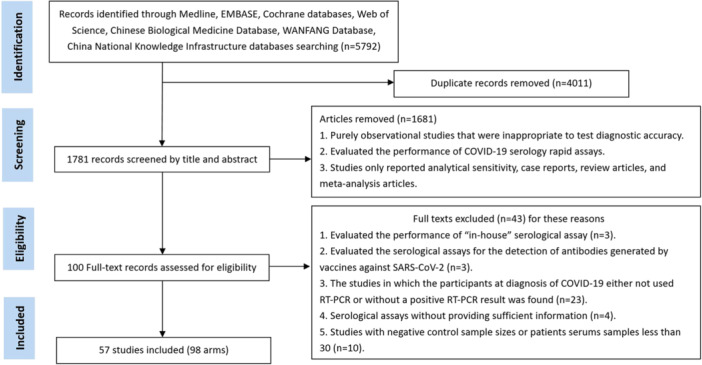
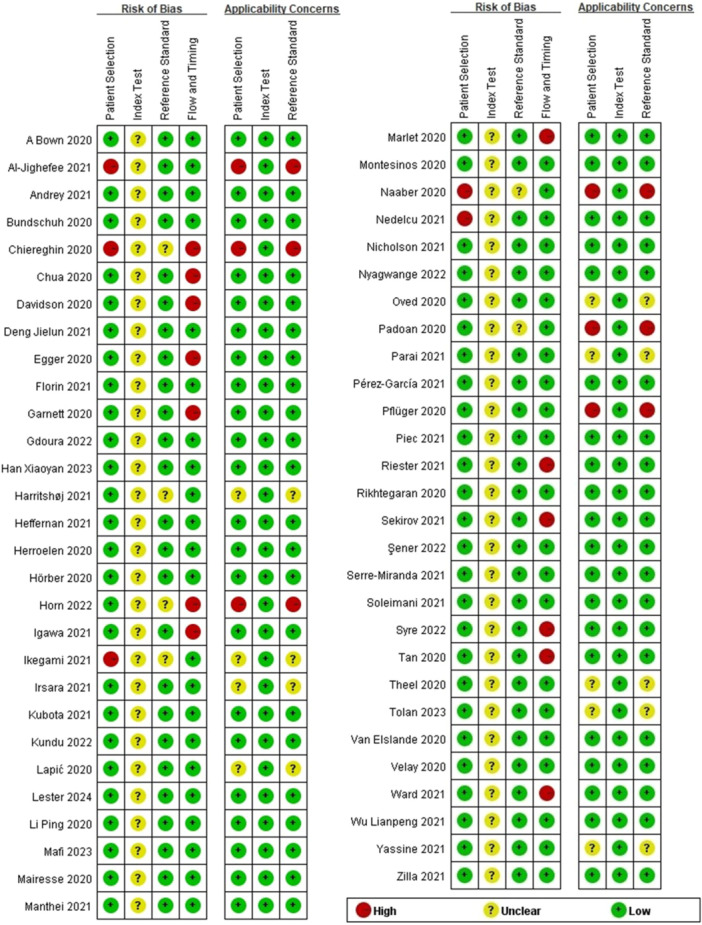
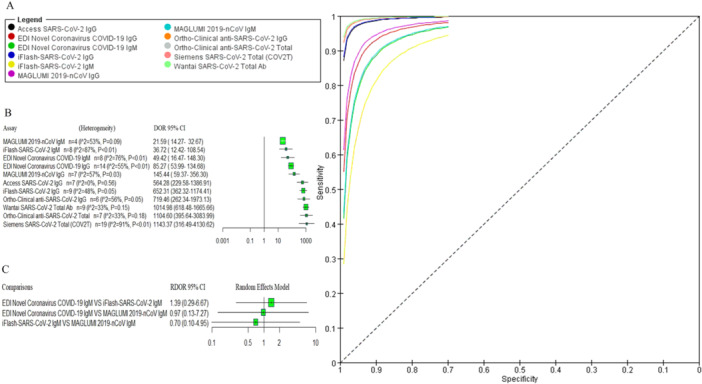
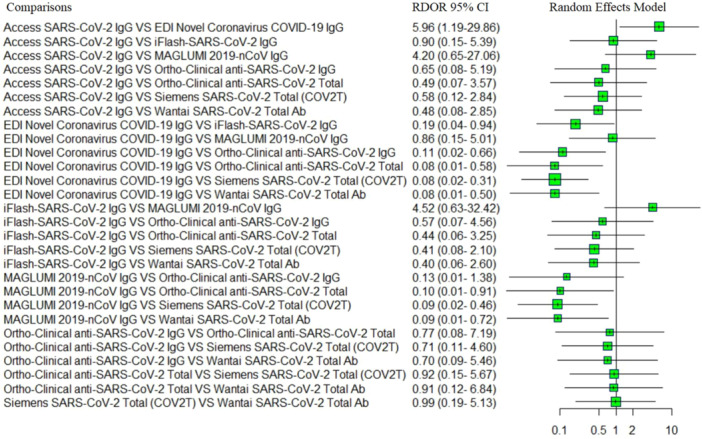
Methods: This meta-analysis was conducted following the PRISMA 2020 reporting guideline. Electronic searches were performed using the Cochrane Library, PubMed, Embase, Web of Science, Chinese Biological Medicine Database (CBM), China National Knowledge Infrastructure (CNKI), WANFANG, and Chinese Weipu (VIP) databases. Fifty-seven articles, including 11 serologic-based IgG, IgM, and total antibodies assays for SARS-CoV-2, published before June 2024, were included in this meta-analysis. The main outcome of this meta-analysis used to evaluate the performance of 11 assays included pooled diagnostic odds ratio (DOR), area under the summary receiver operating characteristic (AUC), and summary receiver operating characteristic curve (SROC). The R software was used for adjusted indirect comparison to calculate the relative diagnostic odds ratio (RDOR) with corresponding 95% confidence intervals (CIs), and indirect comparison forest plots showed the results.
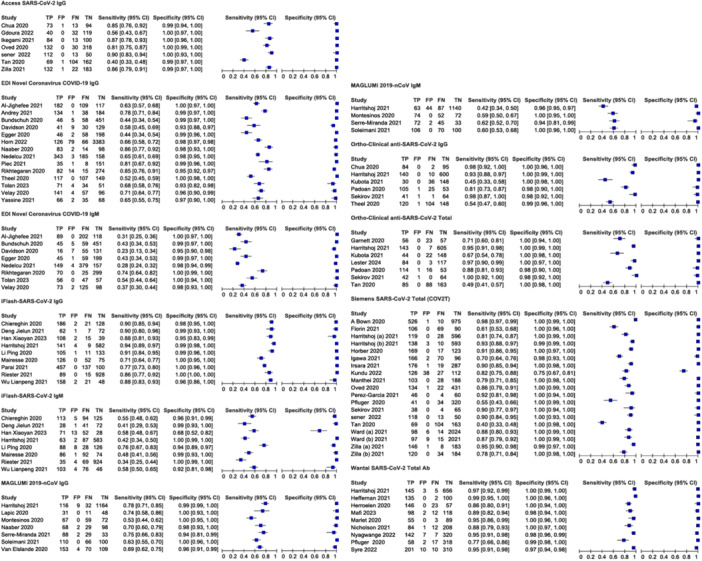
Results: A total of 57 articles met the eligibility criteria for inclusion in our meta-analysis. The pooled DOR and the AUC for access SARS-CoV-2 IgG were 564.28 (95% CI 229.58-1386.91) and 1.00, and as for EDI novel coronavirus COVID-19 IgG those were 85.27 (95% CI 53.99-134.68) and 0.95, for EDI novel coronavirus COVID-19 IgM were 49.42 (95% CI 16.47-148.30) and 0.86, for iFlash-SARS-CoV-2 IgG were 652.31 (95% CI 362.32-1174.41) and 0.97, for iFlash-SARS-CoV-2 IgM were 36.72 (95% CI 12.42-108.54) and 0.76, for MAGLUMI 2019-nCoV IgG were 145.44 (95% CI 59.37-356.30) and 0.90, for MAGLUMI 2019-nCoV IgM were 21.59 (95% CI 14.27-32.67) and 0.59, for ortho-clinical anti-SARS-CoV-2 IgG were 719.46 (95% CI 262.34-1973.13) and 1.00, for ortho-clinical anti-SARS-CoV-2 total were 1104.60 (95% CI 395.64-3083.99) and 1.00, for Siemens SARS-CoV-2 total (COV2T) were 1143.37 (95% CI 316.49-4130.62) and 0.99, for Wantai SARS-CoV-2 total Ab were 1014.98 (95% CI 618.48-1665.66) and 1.00. The pooled DOR for assays-based IgG (n = 43), assays-based total antibody (n = 35), and assays-based IgM (n = 20) was 242.88 (95% CI 157.66-374.16), 1215.90 (95% CI 547.14-2702.07), and 40.99 (95% CI 22.63-74.25). The diagnostic accuracy of assays-based total antibody performed better than those of assays-based IgG and assays-based IgM; assays-based IgG performed better than assays-based IgM.
Conclusion: This study suggested that the Siemens SARS-CoV-2 total (COV2T), ortho-clinical anti-SARS-CoV-2 total, and Wantai SARS-CoV-2 total had the best overall diagnostic accuracy. The diagnostic efficacy of the assays-based total antibody had statistically significantly higher accuracy than those of assays-based IgG and assays-based IgM for COVID-19.
Keywords: COVID‐19; SARS‐CoV2; adjusted indirect comparison; meta‐analysis; serological assays.
© 2024 The Author(s). Immunity, Inflammation and Disease published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Braun J., Loyal L., Frentsch M., et al., “SARS‐CoV‐2‐Reactive T Cells in Healthy Donors and Patients With COVID‐19,” Nature 587, no. 7833 (2020): 270–274. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
