

A two-stage model for precise identification and Gleason grading of clinically significant prostate cancer: a hybrid approach
- PMID: 39698957
- PMCID: PMC11909710
- DOI: 10.1002/jmrs.841
A two-stage model for precise identification and Gleason grading of clinically significant prostate cancer: a hybrid approach
Abstract
Introduction: Accurate identification and grading of clinically significant prostate cancer (csPCa, Gleason Score ≥ 7) without invasive procedures remains a significant clinical challenge. This study aims to develop and evaluate a two-stage model designed for precise Gleason grading. The model initially uses radiomics-based multiparametric MRI to identify csPCa and then refines the Gleason grading by integrating clinical indicators and radiomics features.
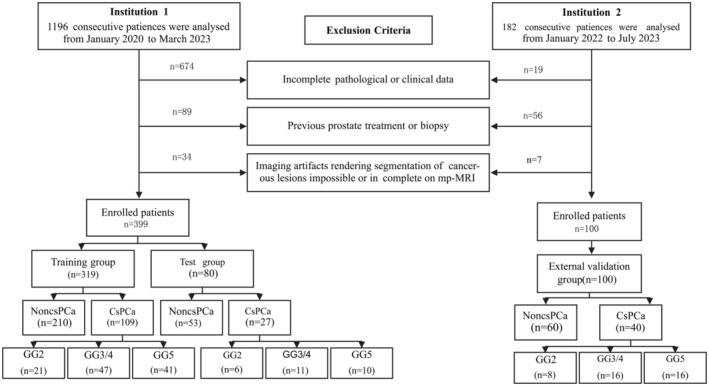
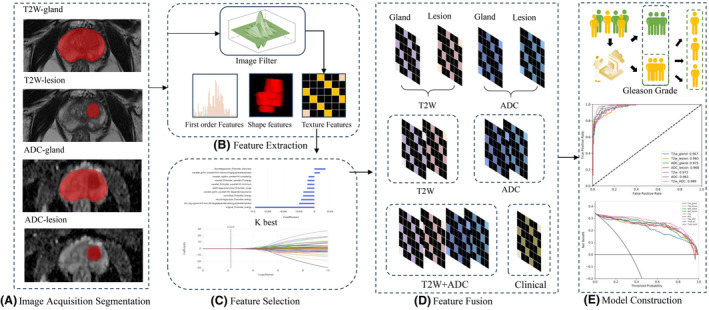
Methods: We retrospectively analysed 399 patients with PI-RADS ≥ 3 lesions, categorising them into non-significant prostate cancer (nsPCa, 263 cases) and csPCa (136 cases, subdivided by GGs). Regions of interest (ROIs) for the prostate and lesions were manually delineated on T2-weighted and apparent diffusion coefficient (ADC) images, followed by the extraction of radiomics features. A two-stage model was developed: the first stage identifies csPCa using radiomics-based MRI, and the second integrates clinical indicators for Gleason grading. Model efficacy was evaluated by sensitivity, specificity, accuracy and area under the curve (AUC), with external validation on 100 patients.
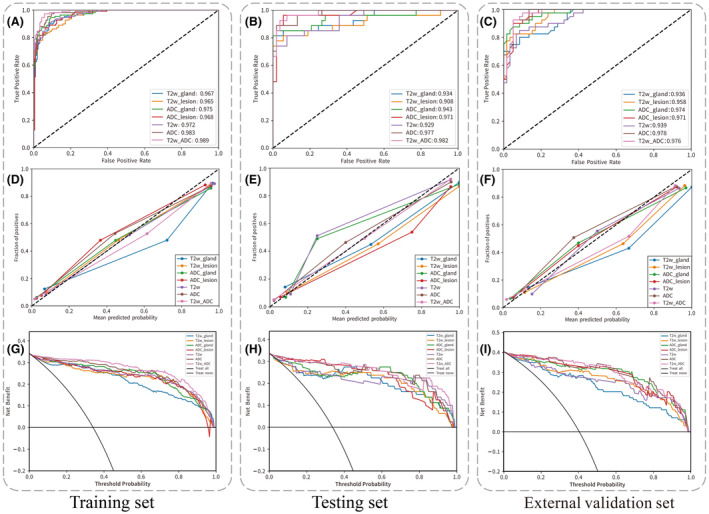
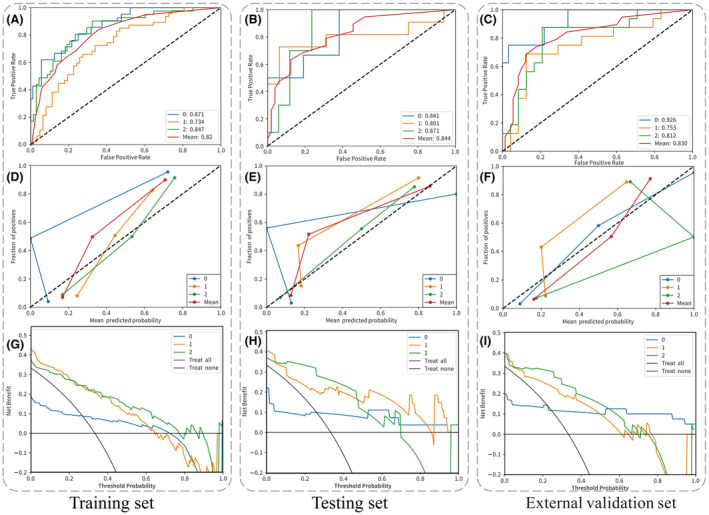
Results: The first-stage model demonstrated excellent diagnostic accuracy for csPCa, achieving AUCs of 0.989, 0.982 and 0.976 in the training, testing and external validation cohorts, respectively. The second-stage model exhibited commendable Gleason grading capabilities, with AUCs of 0.82, 0.844 and 0.83 across the same cohorts. Decision curve analysis supported the clinical applicability of both models.
Conclusions: This study validated the potential of T2W and ADC image radiomics features as biomarkers in distinguishing csPCa. Combining these features with clinical indicators for csPCa Gleason grading provides superior predictive performance and significant clinical benefit.
Keywords: Clinically significant prostate cancer (csPCa); Gleason grading; multiparametric MRI (mpMRI); prostate cancer (PCa); radiomics.
© 2024 The Author(s). Journal of Medical Radiation Sciences published by John Wiley & Sons Australia, Ltd on behalf of Australian Society of Medical Imaging and Radiation Therapy and New Zealand Institute of Medical Radiation Technology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gandaglia G, Leni R, Bray F, et al. Epidemiology and prevention of prostate cancer. Eur Urol Oncol 2021; 4: 877–892. - PubMed
-
- Iczkowski KA, van Leenders G, van der Kwast TH. The 2019 International Society of Urological Pathology (ISUP) consensus conference on grading of prostatic carcinoma. Am J Surg Pathol 2021; 45: 1007. - PubMed
-
- Cornford P, van den Bergh RCN, Briers E, et al. EAU‐EANM‐ESTRO‐ESUR‐SIOG guidelines on prostate cancer. Part II‐2020 update: treatment of relapsing and metastatic prostate cancer. Eur Urol 2021; 79: 263–282. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
