

Prevalence of Mitral Annular Disjunction at Cardiac MRI: Results from a Multicenter Registry
- PMID: 39699304
- PMCID: PMC11683205
- DOI: 10.1148/ryct.230428
Prevalence of Mitral Annular Disjunction at Cardiac MRI: Results from a Multicenter Registry
Abstract
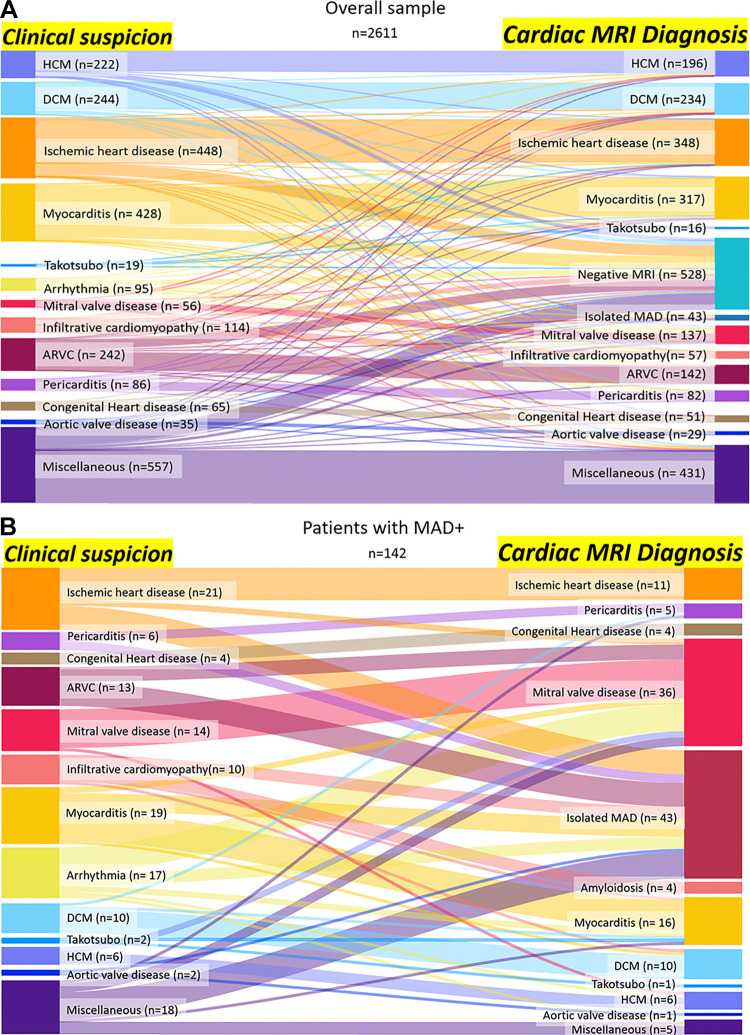
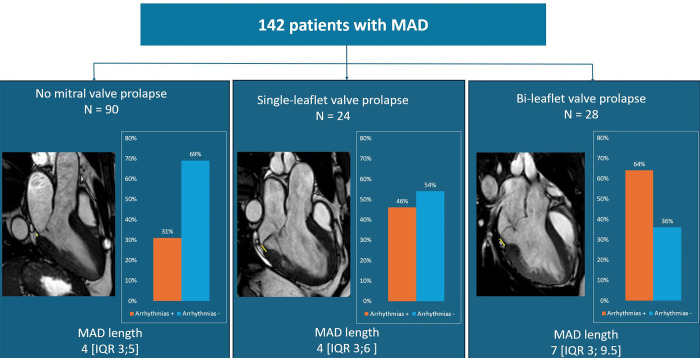
Purpose To determine the prevalence of mitral annular disjunction (MAD) in patients undergoing cardiac MRI for various clinical indications and to assess the association of MAD with arrhythmia, mitral valve prolapse (MVP), and myocardial alteration. Materials and Methods This study analyzed data from a retrospective observational registry of consecutive patients undergoing cardiac MRI for different clinical indications. Cardiac MRI examinations were performed from January 2019 to June 2019 at 13 Italian hospitals. Images underwent double reading by expert cardiac radiologists from the enrolling center and the core laboratory to assess the presence of MAD. Presence and maximum length of MAD and its association to MVP pattern, functional and structural myocardial alteration, and arrhythmia were evaluated using nonparametric and parametric tests. Logistic regression models were used to identify predictors of arrhythmia. Results Cardiac MRI studies from 2611 consecutive patients (1730, 66% male; median age, 53 years; IQR, 39-65 years) were evaluated. Prevalence of MAD was 5.44% (142 of 2611). MAD was an incidental finding in 74.6% (106 of 142) of patients. Patients with MAD had a higher prevalence of arrhythmias compared with patients without MAD (40% [57 of 142] vs 18% [444 of 2469]; P < .001). Patients with MAD and bileaflet MVP showed a longer MAD compared with patients with single-leaflet or absent MVP (median, 7 mm [IQR, 3-9.5 mm] vs 4 mm [IQR, 3-5 mm]; P < .001), a higher prevalence of systolic curling (75% [21 of 28] vs 30.7% [35 of 114]; P < .001), higher extracellular volume values (30% [IQR, 28%-32%] vs 27% [IQR, 25%-30%]; P = .04), and a higher prevalence of arrhythmia (64.2% [18 of 28] vs 34.2% [39 of 114]; P = .006). MAD length of at least 5 mm was an independent predictor of arrhythmia (odds ratio 3.96; 95% CI: 1.93, 8.15; P < .001). Conclusion MAD was a frequent incidental finding on cardiac MRI scans from a multicenter registry. MAD length of at least 5 mm and coexisting bileaflet MVP showed a higher risk of arrhythmia. Keywords: MR Imaging, Cardiac, Mitral Annular Disjunction Supplemental material is available for this article. ©RSNA, 2024.
Keywords: Cardiac; MR Imaging; Mitral Annular Disjunction.
Conflict of interest statement
Figures



References
-
- Bennett S , Tafuro J , Duckett S , et al. . Definition, prevalence, and clinical significance of mitral annular disjunction in different patient cohorts: A systematic review . Echocardiography 2022. ; 39 ( 3 ): 514 – 523 . - PubMed
-
- Faletra FF, Leo LA, Paiocchi VL, et al. . Morphology of Mitral Annular Disjunction in Mitral Valve Prolapse . J Am Soc Echocardiogr 2022. ; 35 ( 2 ): 176 – 186 . - PubMed
-
- Dejgaard LA, Skjølsvik ET, Lie ØH, et al. . The Mitral Annulus Disjunction Arrhythmic Syndrome . J Am Coll Cardiol 2018. ; 72 ( 14 ): 1600 – 1609 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
