

Intracranial complications in adult patients with severe pneumococcal meningitis: a retrospective multicenter cohort study
- PMID: 39699714
- PMCID: PMC11659536
- DOI: 10.1186/s13613-024-01405-z
Intracranial complications in adult patients with severe pneumococcal meningitis: a retrospective multicenter cohort study
Abstract
Background: We aimed to investigate the association of intracranial complications diagnosed on neuroimaging with neurological outcomes of adults with severe pneumococcal meningitis.
Methods: We performed a retrospective multicenter study on consecutive adults diagnosed with pneumococcal meningitis requiring at least 48 h of stay in the intensive care unit (ICU) and undergoing neuroimaging, between 2005 and 2021. All neuroimaging were reanalyzed to look for intracranial complications which were categorized as (1) ischemic lesion, (2) intracranial hemorrhage (3) abscess/empyema, (4) ventriculitis, (5) cerebral venous thrombosis, (6) hydrocephalus, (7) diffuse cerebral oedema. The primary outcome was unfavorable outcome at 90 days after ICU admission, defined by a modified Rankin Scale (mRS) score > 2.
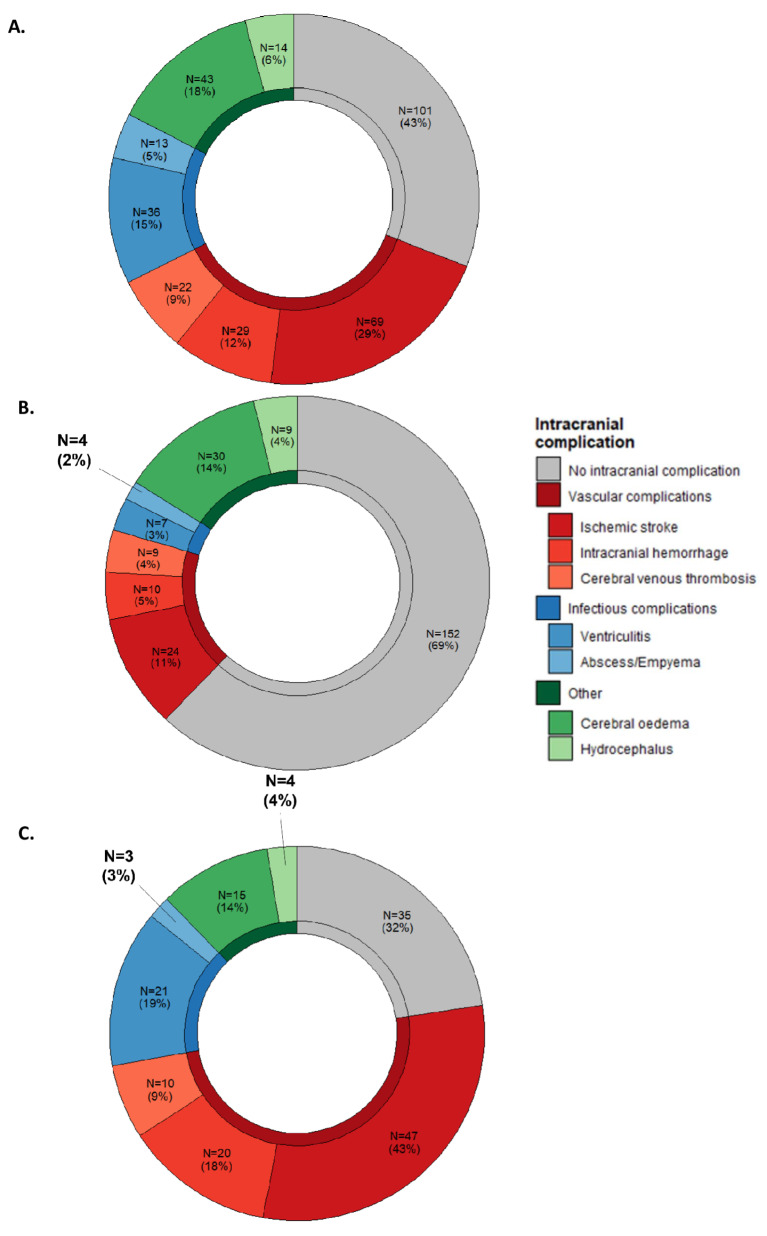
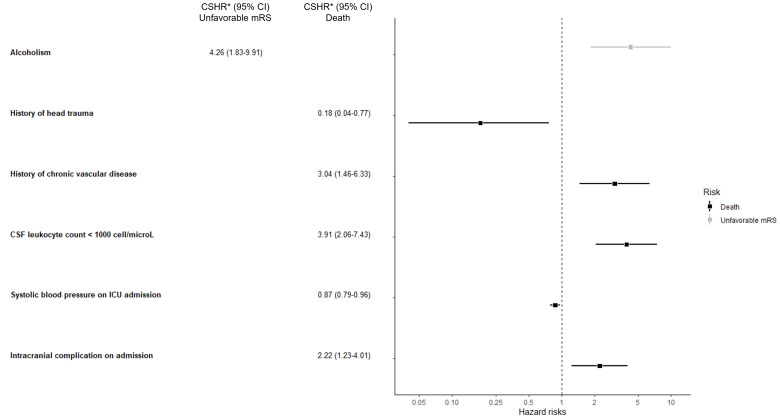
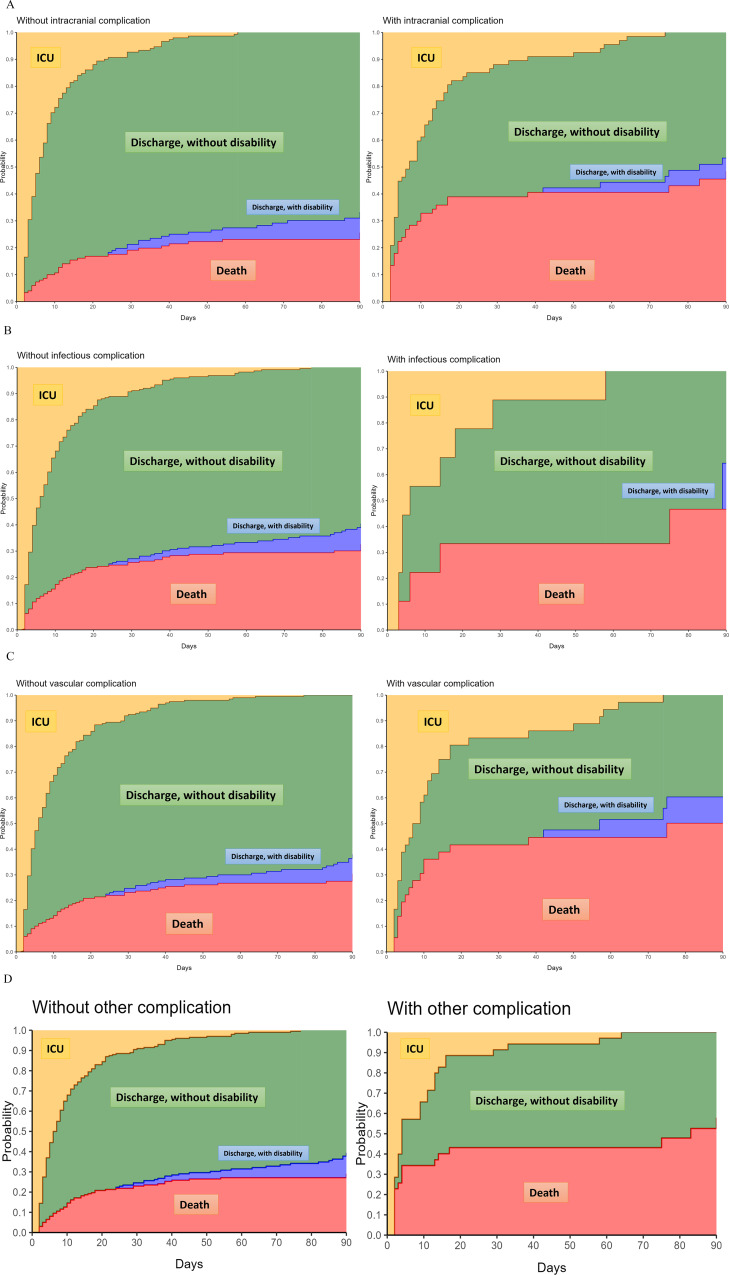
Results: Among the 237 patients included, intracranial complications were diagnosed in 68/220 patients (31%, 95%CI 0.25-0.37) who underwent neuroimaging at ICU admission and in 75/110 patients (68%, 95%CI 0.59-0.77) who underwent neuroimaging during ICU stay. At 90 days, 103 patients (44%, 95%CI 37-50) had unfavorable outcome, including 71 (30%) deaths. The most frequent intracranial complications were ischemic lesion (69/237 patients, 29%), diffuse cerebral oedema (43/237, 18%) and ventriculitis (36/237, 15%). Through multivariable analysis, we found that intracranial complications (adjusted odds ratio (aOR) 2.88, 95%CI 1.37-6.21) were associated with unfavorable outcome, along with chronic alcohol consumption (aOR 3.10, 95%CI 1.27-7.90), chronic vascular disease (aOR 4.41, 95%CI 1.58-13.63), focal neurological sign(s) (aOR 2.38, 95%CI 1.11-5.23), and cerebrospinal fluid leukocyte count < 1000 cell/microL (aOR 4.24, 95%CI 2.11-8.83). Competing risk analysis, with persistent disability (mRS score 3-5) as the primary risk and ICU-death as the competing risk, revealed that chronic alcohol consumption was the sole significant variable associated with persistent disability at 90 days (cause-specific hazard ratio 4.26, 95%CI 1.83-9.91), whereas the remaining variables were associated with mortality.
Conclusions: In adults with severe pneumococcal meninigitis, intracranial complications were independently associated with a higher risk of poor functional outcome, in the form of persistent disability or death. This study highlights the value of neuroimaging studies in this population, and provides relevant information for prognostication.
Keywords: Intensive care unit; Intracranial complications; Neurology; Neuropronostication; Pneumococcal meningitis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol named PNEUMATICS was approved for all participating sites by the French regulatory authorities CNIL (Commission Nationale de l’Informatique et des Libertés, n°922134) on June 30, 2022 and the local ethic committee (CLEA-2021-209). Procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975. Consent for publication: Not applicable. Competing interests: RS received research grants from the French Ministry of Health and from LFB.
Figures

References
LinkOut - more resources
Full Text Sources
