

Circulating cytokine associations with clinical outcomes in melanoma patients treated with combination nivolumab plus ipilimumab
- PMID: 39699928
- PMCID: PMC11660408
- DOI: 10.1080/2162402X.2024.2432723
Circulating cytokine associations with clinical outcomes in melanoma patients treated with combination nivolumab plus ipilimumab
Abstract
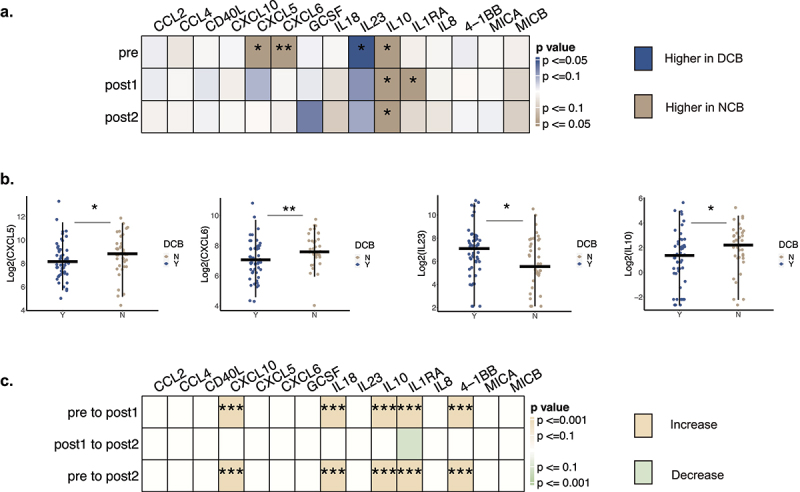
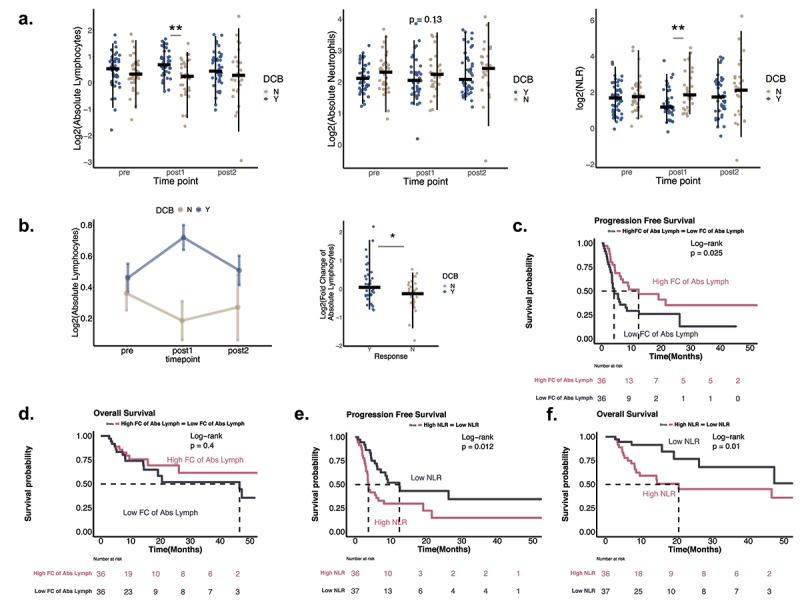
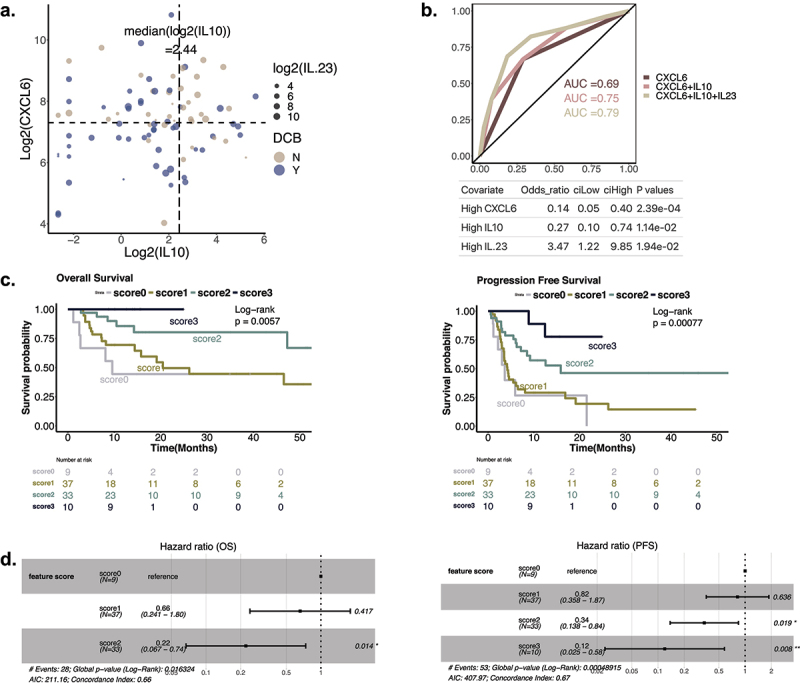
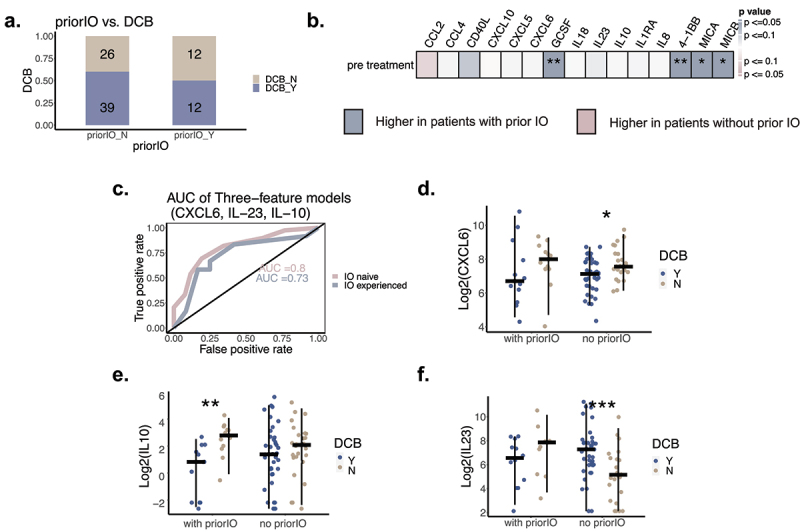
Nivolumab plus ipilimumab (aCTLA-4/aPD-1) combination therapy has significantly improved clinical outcomes in patients with metastatic melanoma, with 50%-60% of patients responding to treatment, but predictors of response are poorly characterized. We hypothesized that circulating cytokines and peripheral white blood cells may predict response to therapy and evaluated 15 cytokines and complete blood counts (CBC with differentials) from 89 patients with advanced melanoma treated with combination therapy from three points in time: pre-treatment, one month and approximately three months after starting therapy. Clinical endpoints evaluated included durable clinical benefit (DCB), progression-free survival (PFS), and overall survival (OS). A parsimonious predictive model was developed to identify cytokines predictors of response to combination therapy. In this study, we found that pre-treatment, patients with DCB had higher IL-23, lower CXCL6, and lower IL-10 levels. Lower NLR one month after starting therapy predicted better PFS and OS, primarily driven by an increase in absolute lymphocytes. A multivariate model demonstrated that baseline CXCL6, IL-10, IL-23 were independent predictors of therapy response, and the combined model has reached an area under the curve (AUC) of 0.79 in prediction of response to combination therapy. Our study identified baseline CXCL6, IL-23, and IL-10 as predictors of response to aCTLA4/aPD1 combination therapy among patients with metastatic melanoma. This study also provides a framework for identifying patients who are likely to respond to combination ICB, as well as a subset of patients with high risk of developing resistance and are thus in need of alternative therapeutic options, such as clinical trials.
Keywords: Checkpoint blockade; biomarkers for immunotherapy; combination immunotherapy; cytokines; melanoma; translational research.
Conflict of interest statement
F. Stephen Hodi receives grants and personal fees from Bristol-Myers Squibb, personal fees from Merck, grants and personal fees from Novartis, personal fees from Surface, personal fees from Compass Therapeutics, personal fees from Apricity, personal fees from Bicara, personal fees from Checkpoint Therapeutics, personal fees from Genentech/Roche, personal fees from Bioentre, personal fees from Gossamer, personal fees from Iovance, personal fees from Catalym, personal fees from Immunocore, personal fees from Kairos, personal fees from Rheos, personal fees from Zumutor, personal fees from Corner Therapeutics, personal fees from Puretech, personal fees from Curis, personal fees from Astra Zeneca, outside the submitted work; In addition, Dr. Hodi has a patent Methods for Treating MICA-Related Disorders (#20100111973) with royalties paid, a patent Tumor antigens and uses thereof (#7250291) issued, a patent Angiopoietin-2 Biomarkers Predictive of Anti-immune checkpoint response (#20170248603) pending, a patent Compositions and Methods for Identification, Assessment, Prevention, and Treatment of Melanoma using PD-L1 Isoforms (#20160340407) pending, a patent Therapeutic peptides (#20160046716) pending, a patent Therapeutic Peptides (#20140004112) pending, a patent Therapeutic Peptides (#20170022275) pending, a patent Therapeutic Peptides (#20170008962) pending, a patent THERAPEUTIC PEPTIDES Therapeutic Peptides Patent number: 9402905 issued, a patent METHODS OF USING PEMBROLIZUMAB AND TREBANANIB pending, a patent Vaccine compositions and methods for restoring NKG2D pathway function against cancers Patent number: 10279021 issued, a patent Antibodies that bind to MHC class I polypeptide-related sequence A Patent number: 10106611 issued, and a patent ANTI-GALECTIN ANTIBODY BIOMARKERS PREDICTIVE OF ANTI-IMMUNE CHECKPOINT AND ANTI-ANGIOGENESIS RESPONSES.
David Liu serves on the scientific advisory board of Oncovalent Therapeutics.
Joanna Baginska declares personal fees from Compass Therapeutics.
Mariano Severgnini is employed by Curis Inc, Boudicca.
Scott J. Rodig receives research support from Bristol Myers Squibb and KITE/Gilead. He is a member of the SAB of Immunitas Therapeutics.
Figures
References
-
- Peres LC, Townsend MK, Birmann BM, Conejo-Garcia JR, Kim Y, Kubzansky LD, Magpantay LI, Martinez-Maza O, Tworoger SS. Circulating biomarkers of inflammation and ovarian cancer risk in the nurses’ health studies. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2021;30(4):710–718. doi:10.1158/1055-9965.EPI-20-1390. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical