Obesity and Polycystic Ovary Syndrome
- PMID: 39701598
- PMCID: PMC11704221
- DOI: 10.7570/jomes24035
Obesity and Polycystic Ovary Syndrome
Abstract
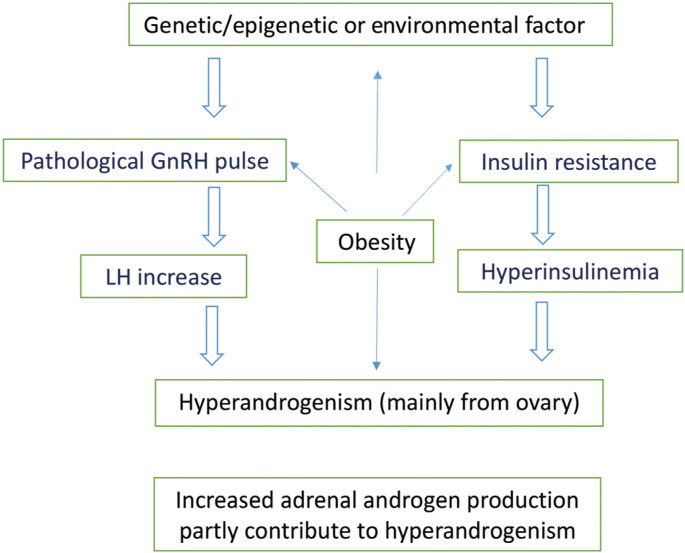
The core pathophysiology of polycystic ovary syndrome involves an overproduction of androgens primarily originating from ovarian thecal cells. Two major external triggers promote androgen overproduction in the ovaries: the increased secretion of luteinizing hormone, a consequence of aberrant hypothalamic gonadotropin-releasing hormone secretion dynamics, and compensatory hyperinsulinemia resulting from insulin resistance. Obesity interacts with polycystic ovary syndrome in multiple ways, but a major role of obesity in its pathophysiology is the exacerbation of insulin resistance. Additionally, obesity contributes to polycystic ovary syndrome by facilitating the conversion of precursor hormones to testosterone within adipose cells. Moreover, obesity can lead to relative hyperandrogenemia, which is marked by lower levels of sex hormone binding globulin and increased availability of free testosterone to target tissues. Also, obesity affects the secretion of gonadotropins, resulting in heightened luteinizing hormone secretion or increased sensitivity of thecal cells to luteinizing hormone. Obesity-related insulin resistance might be amplified by alterations in adipokine and inflammatory cytokine production. Ultimately, obesity and polycystic ovary syndrome might share a common genetic predisposition. The cornerstone of managing polycystic ovary syndrome is to address individual symptoms such as hyperandrogenism (hirsutism, acne, and female type boldness), menstrual irregularities, and infertility stemming from anovulation. However, obesity is integral to the pathophysiology of polycystic ovary syndrome and exacerbates all of its features. Therefore, lifestyle modifications aimed at weight reduction should be the primary strategy in overweight or obese women with polycystic ovary syndrome.
Keywords: Anovulation; Insulin resistance; Obesity; Polycystic ovary syndrome.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources