

Artificial intelligence tools for engagement prediction in neuromotor disorder patients during rehabilitation
- PMID: 39702317
- PMCID: PMC11657850
- DOI: 10.1186/s12984-024-01519-2
Artificial intelligence tools for engagement prediction in neuromotor disorder patients during rehabilitation
Abstract
Background: Robot-Assisted Gait Rehabilitation (RAGR) is an established clinical practice to encourage neuroplasticity in patients with neuromotor disorders. Nevertheless, tasks repetition imposed by robots may induce boredom, affecting clinical outcomes. Thus, quantitative assessment of engagement towards rehabilitation using physiological data and subjective evaluations is increasingly becoming vital. This study aimed at methodologically exploring the performance of artificial intelligence (AI) algorithms applied to structured datasets made of heart rate variability (HRV) and electrodermal activity (EDA) features to predict the level of patient engagement during RAGR.
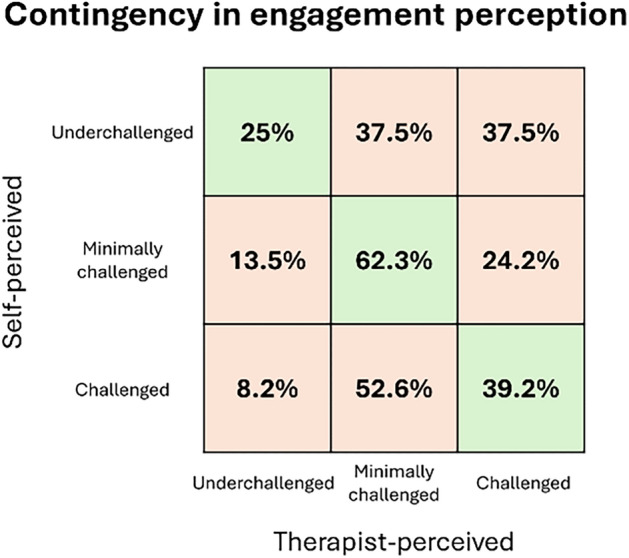
Methods: The study recruited 46 subjects (38 underage, 10.3 ± 4.0 years old; 8 adults, 43.0 ± 19.0 years old) with neuromotor impairments, who underwent 15 to 20 RAGR sessions with Lokomat. During 2 or 3 of these sessions, ad hoc questionnaires were administered to both patients and therapists to investigate their perception of a patient's engagement state. Their outcomes were used to build two engagement classification targets: self-perceived and therapist-perceived, both composed of three levels: "Underchallenged", "Minimally Challenged", and "Challenged". Patient's HRV and EDA physiological signals were processed from raw data collected with the Empatica E4 wristband, and 33 features were extracted from the conditioned signals. Performance outcomes of five different AI classifiers were compared for both classification targets. Nested k-fold cross-validation was used to deal with model selection and optimization. Finally, the effects on classifiers performance of three dataset preparation techniques, such as unimodal or bimodal approach, feature reduction, and data augmentation, were also tested.
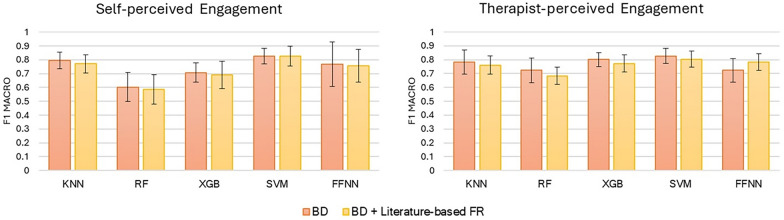
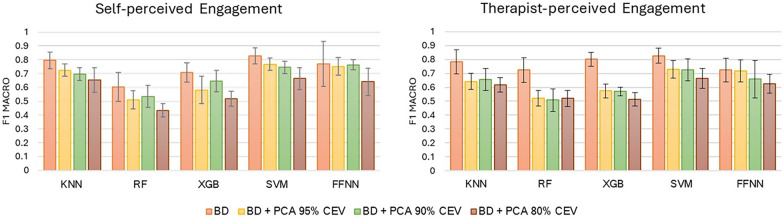
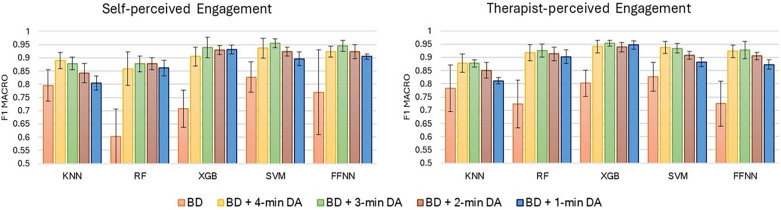
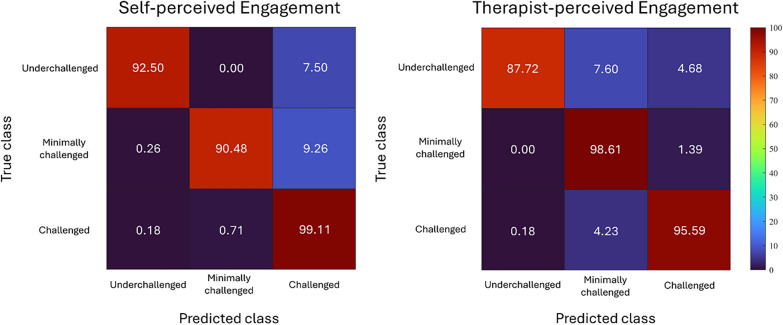
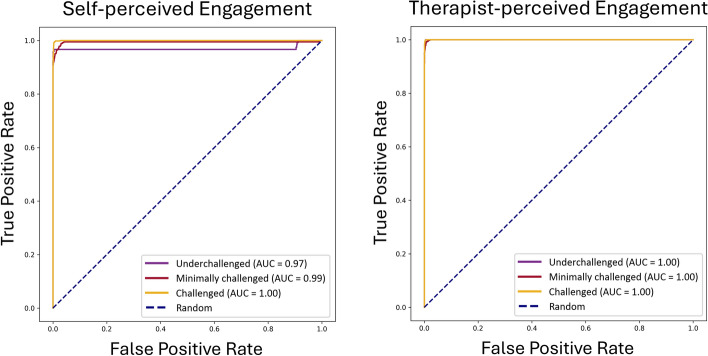
Results: The study found that combining HRV and EDA features into a comprehensive dataset improved the synergistic representation of engagement compared to unimodal datasets. Additionally, feature reduction did not yield any advantages, while data augmentation consistently enhanced classifiers performance. Support Vector Machine and Extreme Gradient Boosting models were found to be the most effective architectures for predicting self-perceived engagement and therapist-perceived engagement, with a macro-averaged F1 score of 95.6% and 95.4%, respectively.
Conclusion: The study displayed the effectiveness of psychophysiology-based AI models in predicting rehabilitation engagement, thus promoting their practical application for personalized care and improved clinical health outcomes.
Keywords: Classification; Engagement; Extreme Gradient Boosting; K-Nearest Neighbors; Neural Network; Psychophysiological signals; Random forest; Robot-Assisted Gait Rehabilitation; Support Vector Machine.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was performed in accordance with the Declaration of Helsinki, and the Ethics Committee of Scientific Institute E. Medea approved the observational study protocol (protocol code: Prot. N. 02/22-CE; date of approval: January 27th, 2022). Patients, if adults, or their guardians signed a written informed consent. Consent for publication: All subjects consented for their data to be published. Competing interests: The authors declare no competing interests.
Figures


References
-
- Valè N, Gandolfi M, Vignoli L, Botticelli A, Posteraro F, Morone G, et al. Electromechanical and robotic devices for gait and balance rehabilitation of children with neurological disability: a systematic review. Appl Sci. 2021;11(24):12061. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
