

Efficacy and safety of tofacitinib in an open-label, long-term extension study in patients with psoriatic arthritis who received adalimumab or tofacitinib in a Phase 3 randomized controlled study: a post hoc analysis
- PMID: 39702318
- PMCID: PMC11657006
- DOI: 10.1186/s13075-024-03442-2
Efficacy and safety of tofacitinib in an open-label, long-term extension study in patients with psoriatic arthritis who received adalimumab or tofacitinib in a Phase 3 randomized controlled study: a post hoc analysis
Abstract
Background: Data on treatment switching directly from tumor necrosis factor inhibitors to tofacitinib in psoriatic arthritis (PsA) are limited. This post hoc analysis assessed efficacy and safety outcomes in patients with PsA who directly switched to tofacitinib in a long-term extension (LTE) study after receiving adalimumab (ADA) in a Phase 3 study, compared with those who continued to receive tofacitinib.
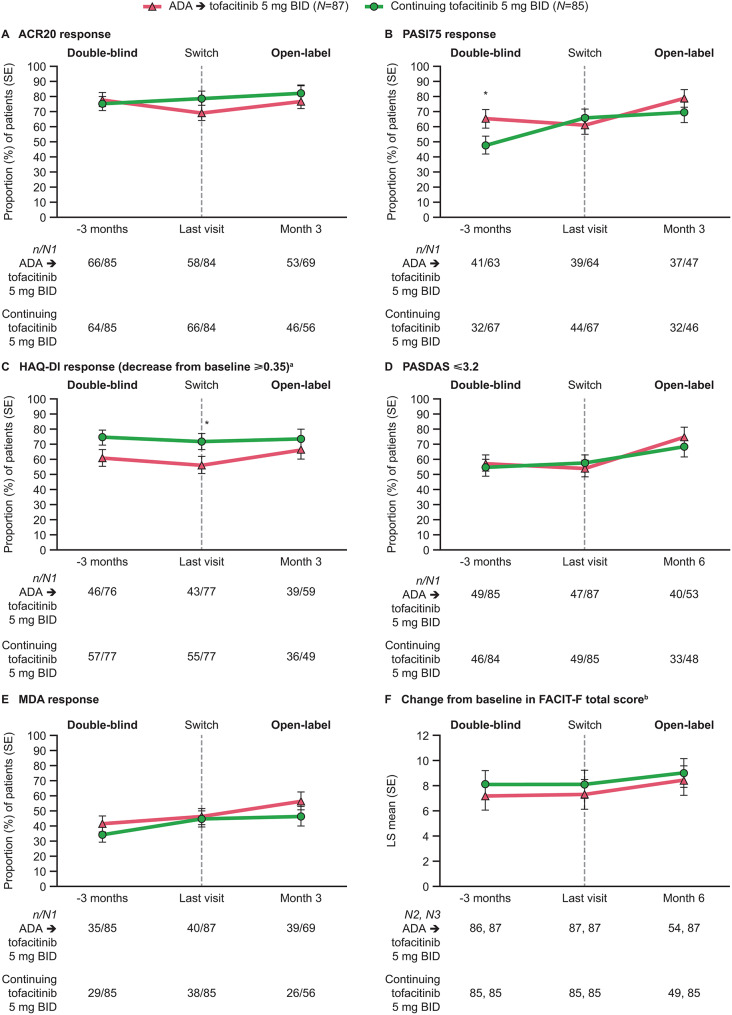
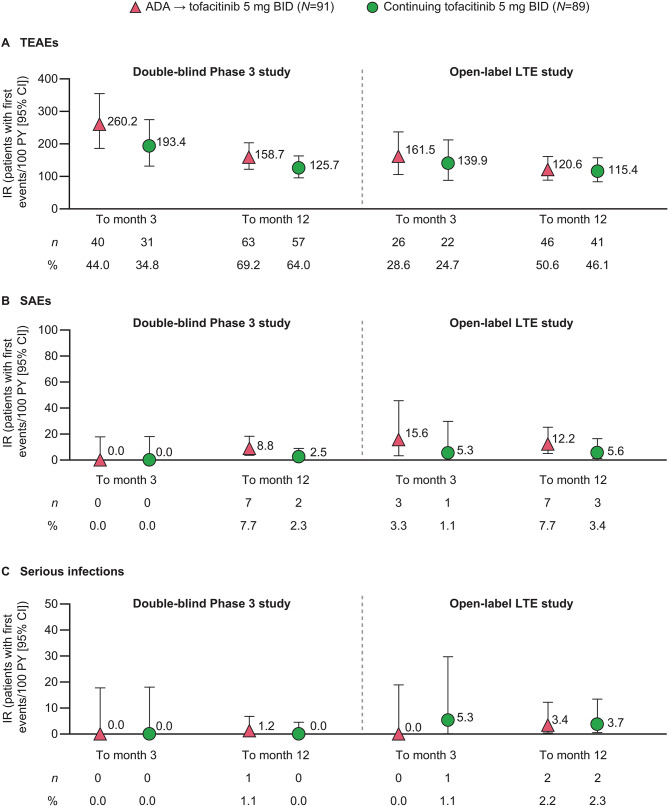
Methods: Patients with active PsA received tofacitinib 5 mg twice daily (BID) or ADA 40 mg once every 2 weeks in a 12-month, randomized, double-blind study (OPAL Broaden) and then continued or switched to tofacitinib 5 mg BID and maintained this dose in an open-label LTE study (OPAL Balance). Efficacy was assessed 3 months before the last visit and at the last visit in the Phase 3 study, and at month 3 (or month 6 for select outcomes) in the LTE study and included rates of ≥ 20/50/70% improvement in American College of Rheumatology response criteria, Psoriasis Area and Severity Index ≥ 75% improvement, Health Assessment Questionnaire-Disability Index (HAQ-DI) response (decrease from baseline ≥ 0.35 for patients with baseline HAQ-DI ≥ 0.35), Psoriatic Arthritis Disease Activity Score ≤ 3.2, and minimal disease activity; and change from baseline in Functional Assessment of Chronic Illness Therapy-Fatigue score. Safety was assessed at months 3 and 12 in both studies via incidence rates (patients with first events/100 patient-years).
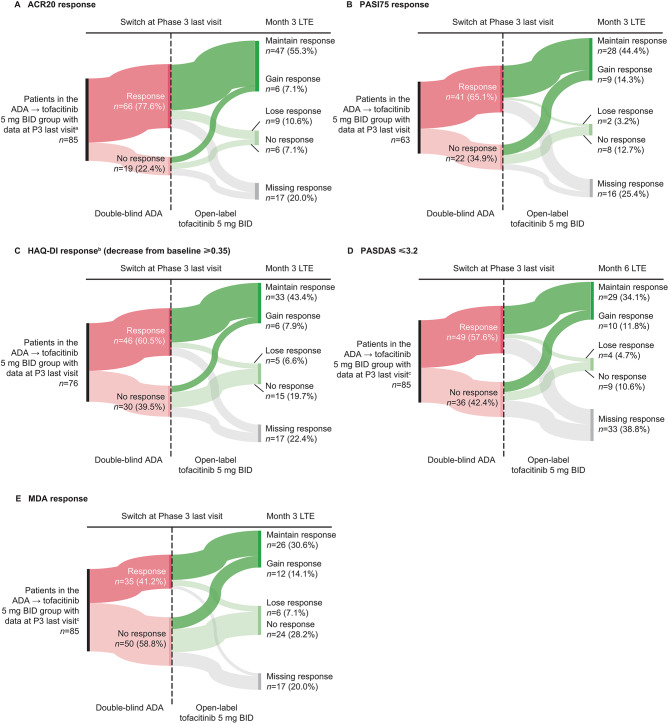
Results: Overall, 180 patients were included (ADA→tofacitinib 5 mg BID: n = 91; continuing tofacitinib 5 mg BID: n = 89). At Phase 3 baseline, patients in the ADA→tofacitinib 5 mg BID group tended to be younger and have less active disease compared with those continuing tofacitinib. Efficacy was similar between groups in the Phase 3 study, and was maintained to month 3 or 6 in the LTE study. Treatment-emergent adverse events (AEs), serious AEs, and serious infections were generally similar in the Phase 3 and LTE studies, and between groups within each study.
Conclusion: Tofacitinib efficacy and safety were similar in patients with PsA who directly switched from ADA to tofacitinib and those who continued tofacitinib, suggesting that patients can be directly switched from ADA to tofacitinib without any washout period.
Trial registration: NCT01877668; NCT01976364.
Keywords: Adalimumab; Psoriatic arthritis; Tofacitinib; Treatment switching.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Both studies were conducted in accordance with the Good Clinical Practice guidelines of the International Council for Harmonisation and with the principles of the Declaration of Helsinki. All patients provided written informed consent and the protocols were approved by the institutional review board or independent ethics committee at each investigational site. Consent for publication: Not applicable. Competing interests: DDG has received grants and/or research support from AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Novartis, Pfizer Inc, and UCB, and has acted as a consultant for AbbVie, Amgen, Bristol Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead Sciences, Janssen, Novartis, Pfizer Inc, and UCB. PN has received grants and/or research support from AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Galapagos, GSK, Janssen, Novartis, Pfizer Inc, and UCB, and has received speaker fees/honoraria from AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Galapagos, GSK, Janssen, Novartis, and Pfizer Inc. PJM has received grants and/or research support from AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead Sciences, Janssen, Novartis, Pfizer Inc, Sun, and UCB, has acted as a consultant for AbbVie, Acelyrin, Aclaris, Alumis, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galapagos, Gilead Sciences, Inmagene, Janssen, MoonLake, Novartis, Pfizer Inc, Sun, UCB, and Ventyx, and has received speaker fees/honoraria from AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer Inc, and UCB. OF has received grants and/or research support from AbbVie, Bristol Myers Squibb, Eli Lilly, Janssen, Novartis, Pfizer Inc, and UCB, has acted as a consultant for Bristol Myers Squibb, Celgene, Eli Lilly, Janssen, and Pfizer Inc, and has received speaker fees/honoraria from AbbVie, Janssen, Novartis, and Pfizer Inc. SD and MJC are employees and stockholders of Pfizer Inc. KRM is a stockholder of Pfizer Inc and was an employee of Pfizer Inc at the time of the analysis.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
