

Age- and sex-related variations in extracellular vesicle profiling for the assessment of cardiovascular risk: the EVaging index
- PMID: 39702460
- PMCID: PMC11659617
- DOI: 10.1038/s41514-024-00189-7
Age- and sex-related variations in extracellular vesicle profiling for the assessment of cardiovascular risk: the EVaging index
Abstract
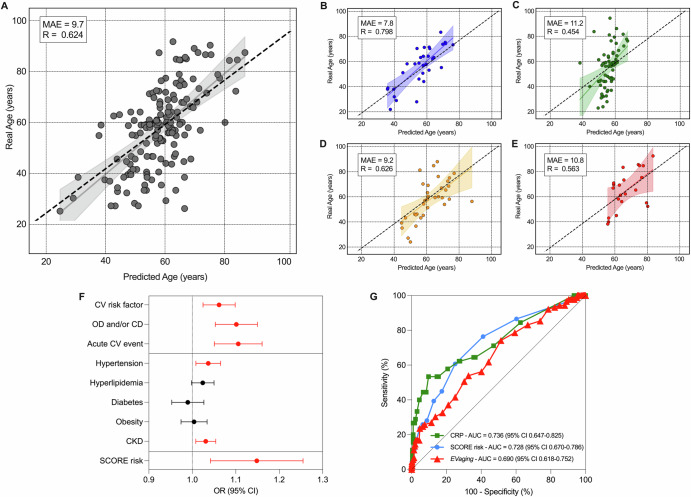
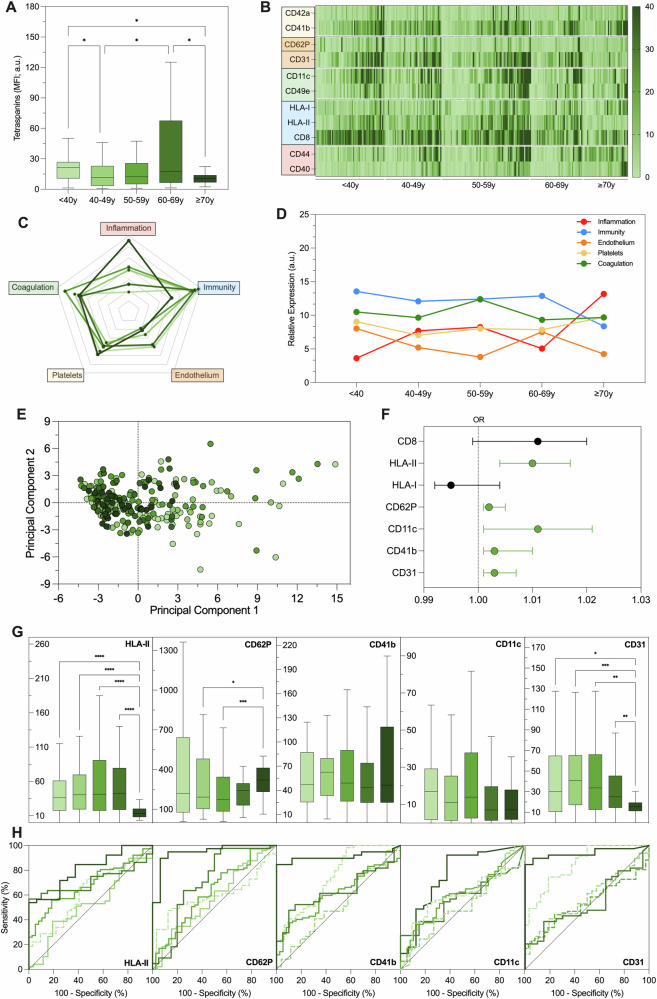
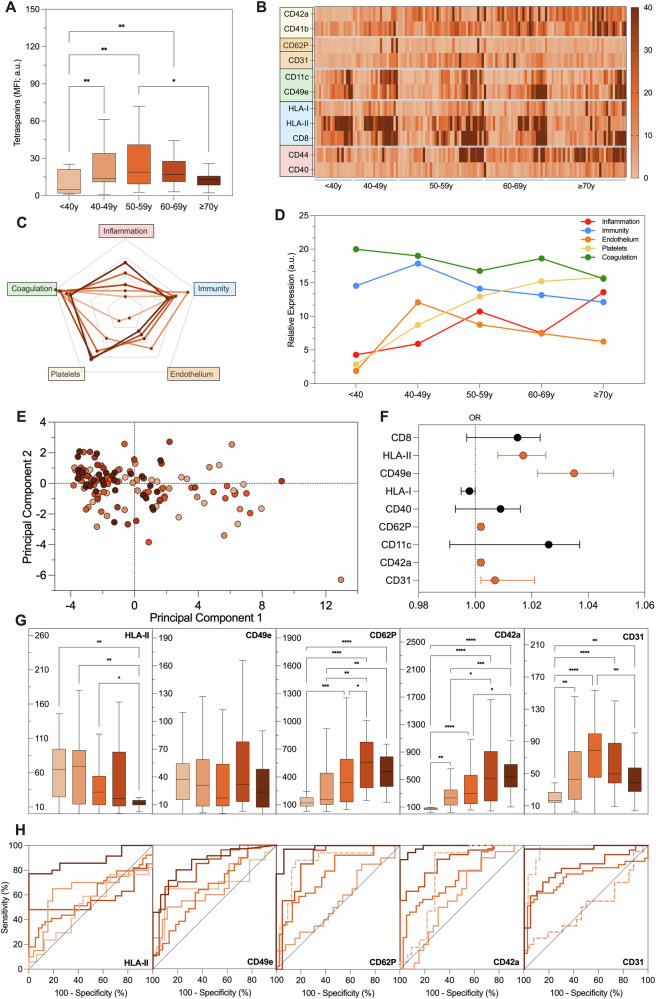
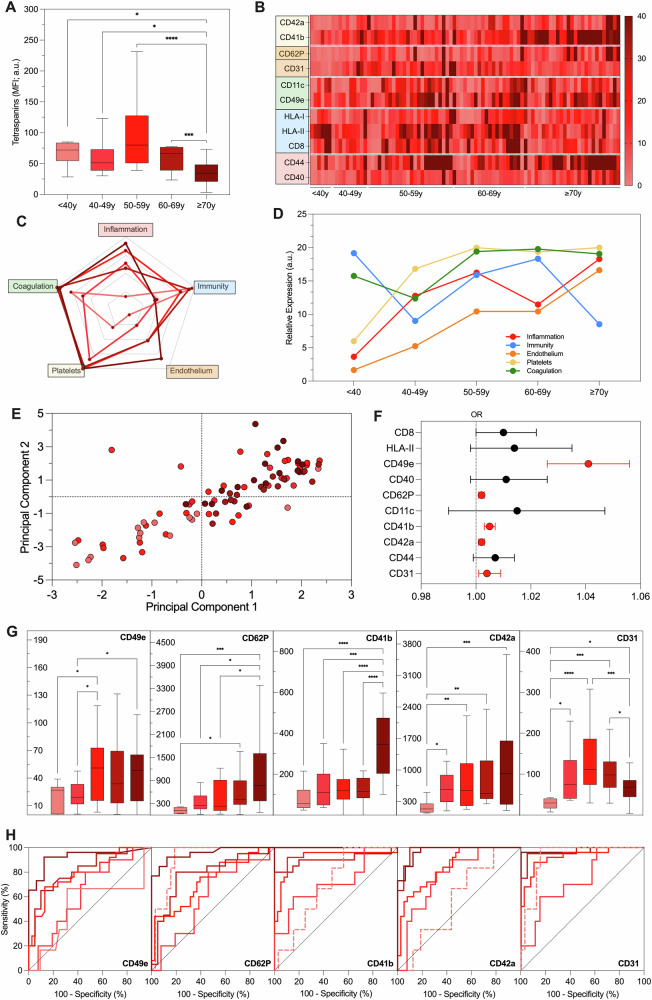
Extracellular vesicles (EVs) offer valuable diagnostic and prognostic insights for cardiovascular (CV) diseases, but the influence of age-related chronic inflammation ("inflammaging") and sex differences on EV profiles linked to CV risk remains unclear. This study aimed to use EV profiling to predict age and stratify patients by CV risk. We developed an EVaging index by analyzing surface antigen profiles of serum EVs from 625 participants, aged 20 to 94 years, across varying CV risk groups. The EVaging index was associated with age in healthy individuals and distinguished CV risk profiles in patients, correlating with CV outcomes and likelihood of fatal CV events according to the European Society of Cardiology (ESC) SCORE, and reflecting age-associated comorbidities. While changes in disease-related EV fingerprint adds complexity in CV patients, EV profiling may help assess biological aging and CV risk, emphasizing EVs' roles in inflammaging.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures

References
-
- Beharka, A. A. et al. Interleukin-6 production does not increase with age. J. Gerontol. A Biol. Sci. Med. Sci.56, B81–B88 (2001). - PubMed
-
- Ahluwalia, N. et al. Cytokine production by stimulated mononuclear cells did not change with aging in apparently healthy, well-nourished women. Mech. Ageing Dev.122, 1269–1279 (2001). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
