

Dual antiplatelet therapy after minor strokes or high-risk TIA: Evidence from the Austrian stroke registry
- PMID: 39702759
- PMCID: PMC11658963
- DOI: 10.1111/ene.70012
Dual antiplatelet therapy after minor strokes or high-risk TIA: Evidence from the Austrian stroke registry
Abstract
Background and purpose: Three large, randomized trials demonstrated the benefit of short-term dual antiplatelet therapy (DAPT) versus monotherapy after non-cardioembolic minor stroke or high-risk transient ischemic attack (TIA). The aim of this study was to evaluate effects of DAPT versus monotherapy on functional outcomes and safety in a real-life setting.
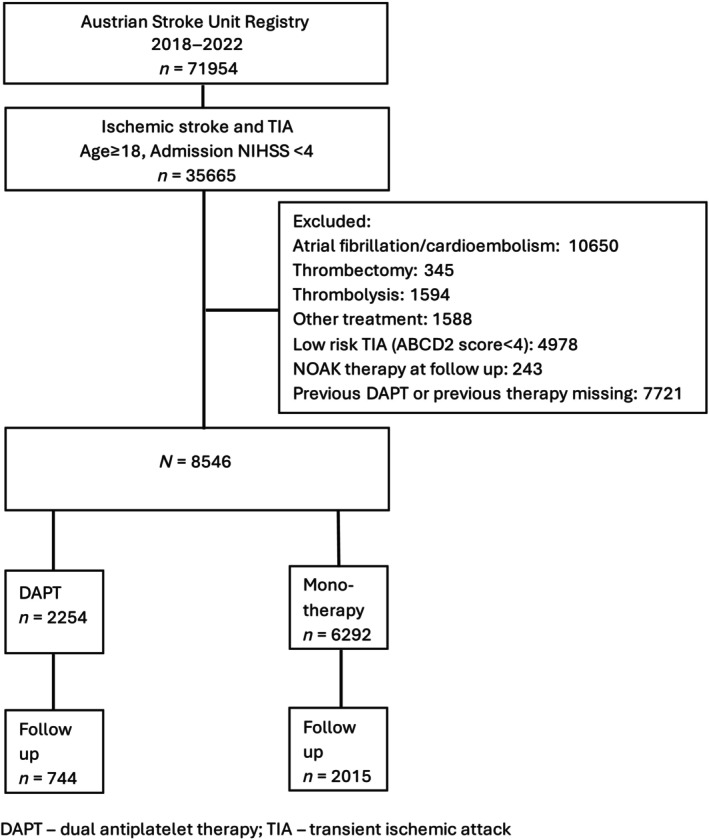
Methods: Patients with minor stroke (NIHSS <4) or high-risk TIA (ABCD2 score ≥4) of non-cardioembolic origin without major vessel occlusion or revascularization therapy (thrombolysis or thrombectomy) treated between 2018 and 2023 were analyzed based on a prospective nationwide stroke unit registry. Data on risk factors, stroke etiology, admission stroke severity (NIHSS), functional status at 3 months (mRS), and mortality were extracted. Excellent functional outcome (mRS 0-1) at 3 months, early neurological deterioration (END), symptomatic intracranial hemorrhage (SICH) and major extracranial bleeds were defined as study endpoints and adjusted for covariates using inverse probability of treatment weighted regression models.
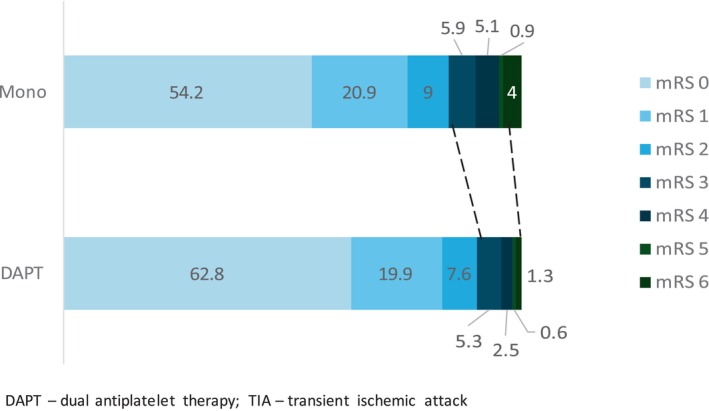
Results: Two Thousand Two Hundred Fifty-four of 8546 patients with non-cardioembolic minor stroke or high-risk TIA received DAPT. Patients treated with DAPT had significantly more risk factors and comorbidities compared to those treated with monotherapy. After robust statistical adjustment, DAPT was significantly associated with lower occurrence of END (OR 0.50 95% CI 0.35-0.72), increased odds of excellent outcome at 3 months (aOR 1.59; 95% CI 1.20-2.09) and equivalent frequencies of SICH (aOR 1.19, 95% CI 0.30-4.73) or major extracranial bleeding (aOR 0.84; 95% CI 0.16-4.56).
Conclusions: DAPT in non-cardioembolic minor stroke or high-risk TIA in a real-life setting appears to be safe and associated with improved functional outcome.
Keywords: dual antiplatelet therapy; minor stroke; outcome.
© 2024 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
The authors declare that there are no conflicts of interest associated with the publication of this article.
Figures
References
-
- Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med. 2013;369:11‐19. - PubMed
-
- Johnston SC, Amarenco P, Denison H, et al. Ticagrelor and aspirin or aspirin alone in acute ischemic stroke or TIA. N Engl J Med. 2020;383:207‐217. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
