

Spatial transcriptomics in breast cancer reveals tumour microenvironment-driven drug responses and clonal therapeutic heterogeneity
- PMID: 39703753
- PMCID: PMC11655296
- DOI: 10.1093/narcan/zcae046
Spatial transcriptomics in breast cancer reveals tumour microenvironment-driven drug responses and clonal therapeutic heterogeneity
Abstract
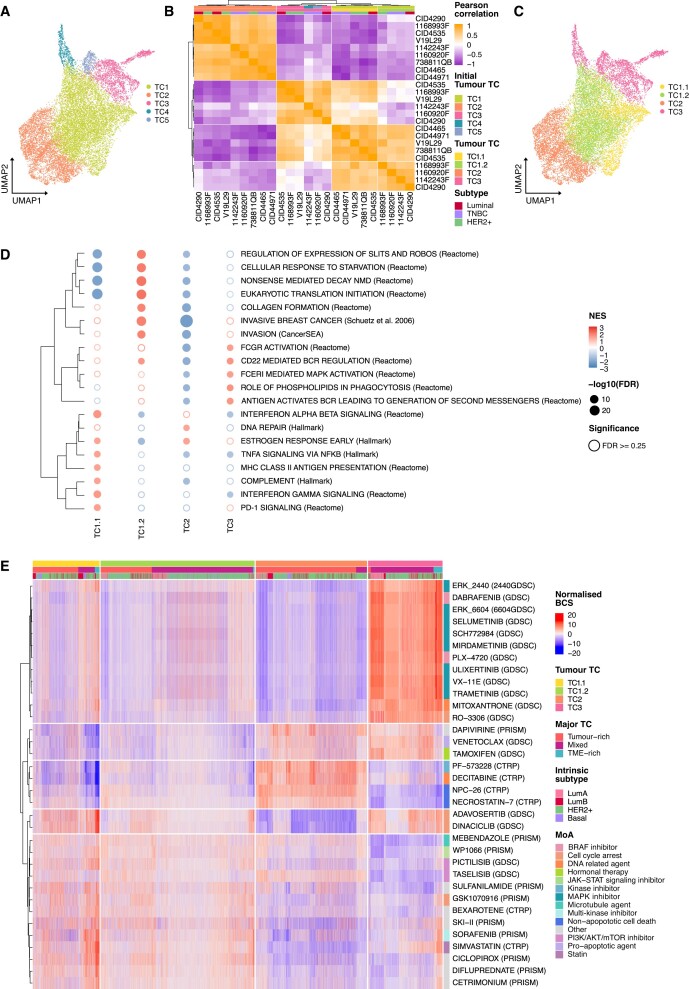
Breast cancer patients are categorized into three subtypes with distinct treatment approaches. Precision oncology has increased patient outcomes by targeting the specific molecular alterations of tumours, yet challenges remain. Treatment failure persists due to the coexistence of several malignant subpopulations with different drug sensitivities within the same tumour, a phenomenon known as intratumour heterogeneity (ITH). This heterogeneity has been extensively studied from a tumour-centric view, but recent insights underscore the role of the tumour microenvironment in treatment response. Our research utilizes spatial transcriptomics data from breast cancer patients to predict drug sensitivity. We observe diverse response patterns across tumour, interphase and microenvironment regions, unveiling a sensitivity and functional gradient from the tumour core to the periphery. Moreover, we find tumour therapeutic clusters with different drug responses associated with distinct biological functions driven by unique ligand-receptor interactions. Importantly, we identify genetically identical subclones with different responses depending on their location within the tumour ducts. This research underscores the significance of considering the distance from the tumour core and microenvironment composition when identifying suitable treatments to target ITH. Our findings provide critical insights into optimizing therapeutic strategies, highlighting the necessity of a comprehensive understanding of tumour biology for effective cancer treatment.
© The Author(s) 2024. Published by Oxford University Press on behalf of NAR Cancer.
Figures





References
-
- Duffy M.J., Crown J. A personalized approach to cancer treatment: how biomarkers can help. Clin. Chem. 2008; 54:1770–1779. - PubMed
-
- Burrell R.A., McGranahan N., Bartek J., Swanton C. The causes and consequences of genetic heterogeneity in cancer evolution. Nature. 2013; 501:338–345. - PubMed
-
- Wahida A., Buschhorn L., Fröhling S., Jost P.J., Schneeweiss A., Lichter P., Kurzrock R. The coming decade in precision oncology: six riddles. Nat. Rev. Cancer. 2023; 23:43–54. - PubMed
LinkOut - more resources
Full Text Sources
