

Community-onset pediatric status epilepticus: Barriers to care and outcomes in a real-world setting
- PMID: 39704293
- PMCID: PMC11908671
- DOI: 10.1111/epi.18216
Community-onset pediatric status epilepticus: Barriers to care and outcomes in a real-world setting
Abstract
Objective: Status epilepticus (SE) is a neurological emergency in childhood, often leading to neuronal damage and long-term outcomes. The study aims to identify barriers in the pre-hospital and in-hospital management of community-onset pediatric SE and to evaluate the effectiveness of pediatric scores on outcomes prediction.
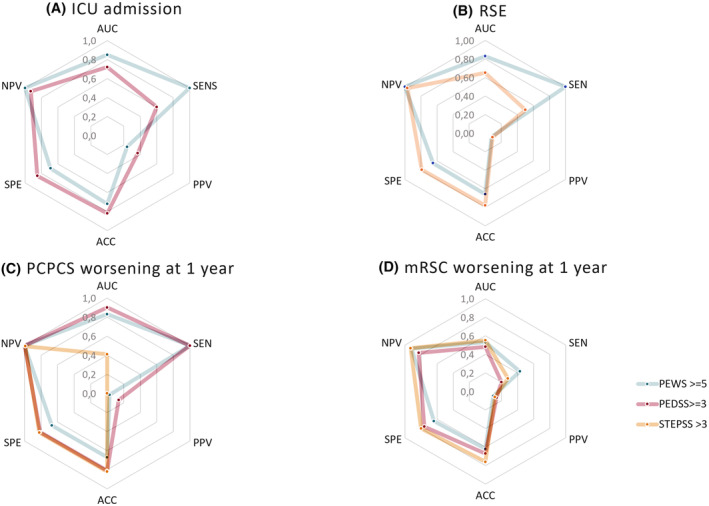
Methods: This monocentric observational retrospective cohort study included patients treated for community-onset pediatric SE in a tertiary care hospital between 2010 and 2021. Data were extracted following Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Inclusion criteria were community-onset SE (according to the International League Against Epilepsy [ILAE] Task Force on SE Classification), admission to the pediatric emergency department (PED), age: 1 month to 18 years. Pre-hospital, in-hospital management and outcomes were analyzed. Pediatric scores for prediction of clinical worsening (Pediatric Early Warning Score - PEWS) and SE outcome (Status Epilepticus in Pediatric patients Severity Score - STEPSS; Pre-status Epilepticus PCPCS, background Electroencephalographic abnormalities, Drug refractoriness, Semiology and critical Sickness Score - PEDSS) were retrospectively assessed for their accuracy in predicting short-term and long-term outcomes.
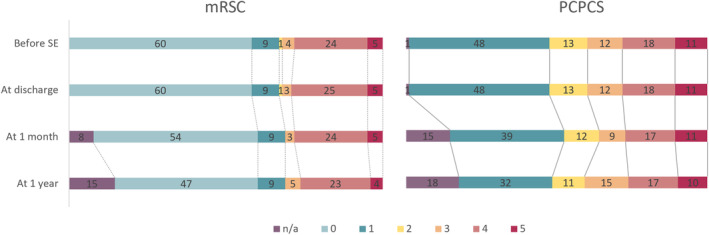
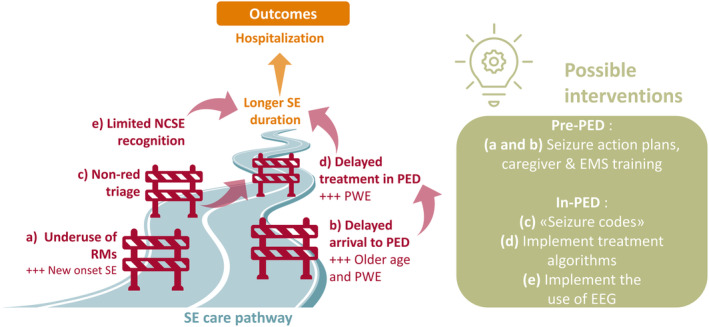
Results: A total of 103 consecutive episodes of SE were included. Out-of-hospital rescue medications administration occurred in 54.4% of cases and was associated with higher SE resolution rate before PED admission (48.2% vs 27.6%, p = .033). Longer in-PED time to treatment was observed in case of delay to PED referral (r = 0.268, p = .048) or non-red triage labels (12 vs 5 min, p = 0.032), and was associated with longer in-PED duration of SE (r = 0.645, p < .001). Longer SE duration was observed in episodes leading to hospitalization compared to those discharged (50 vs 16 min, p < .001). In-PED electroencephalography (EEG) recordings were available in 39.8% of events. Predictive scores varied in accuracy, with PEWS ≥5 showing high sensitivity for intensive care unit (ICU) admission but low specificity. No patients died, 6.3% of SE was refractory.
Significance: Effective pre-hospital administration of rescue medications and prompt PED management are crucial to reduce SE duration and improve outcomes. Predictive scores can aid in assessment of the severity and prognosis of SE; their utility is still not defined. Identifying and addressing actionable care barriers in SE management pathways is essential to enhance patient outcomes in pediatric SE.
Keywords: childhood; management; outcomes; seizures; treatment.
© 2024 The Author(s). Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
The authors declare they have no conflicts of interest to disclose for this work. The local ethics committee was advised of the study.
Figures
References
-
- Trinka E, Cock H, Hesdorffer D, Rossetti AO, Scheffer IE, Shinnar S, et al. A definition and classification of status epilepticus—report of the ILAE task force on classification of status epilepticus. Epilepsia. 2015;56(10):1515–1523. - PubMed
-
- Govoni V, Fallica E, Monetti VC, Guerzoni F, Faggioli R, Casetta I, et al. Incidence of status epilepticus in southern Europe: a population study in the Health District of Ferrara. Italy European Neurology. 2007;59(3–4):120–126. - PubMed
-
- Chin RFM, Neville BGR, Peckham C, Bedford H, Wade A, Scott RC. Incidence, cause, and short‐term outcome of convulsive status epilepticus in childhood: prospective population‐based study. Lancet. 2006;368:1328. - PubMed
-
- Nishiyama I, Ohtsuka Y, Tsuda T, Inoue H, Kunitomi T, Shiraga H, et al. An epidemiological study of children with status epilepticus in Okayama. Japan Epilepsia. 2007;48(6):1133–1137. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
