

Clinical and biochemical features of atherogenic hyperlipidemias with different genetic basis: A comprehensive comparative study
- PMID: 39705280
- PMCID: PMC11661581
- DOI: 10.1371/journal.pone.0315693
Clinical and biochemical features of atherogenic hyperlipidemias with different genetic basis: A comprehensive comparative study
Abstract
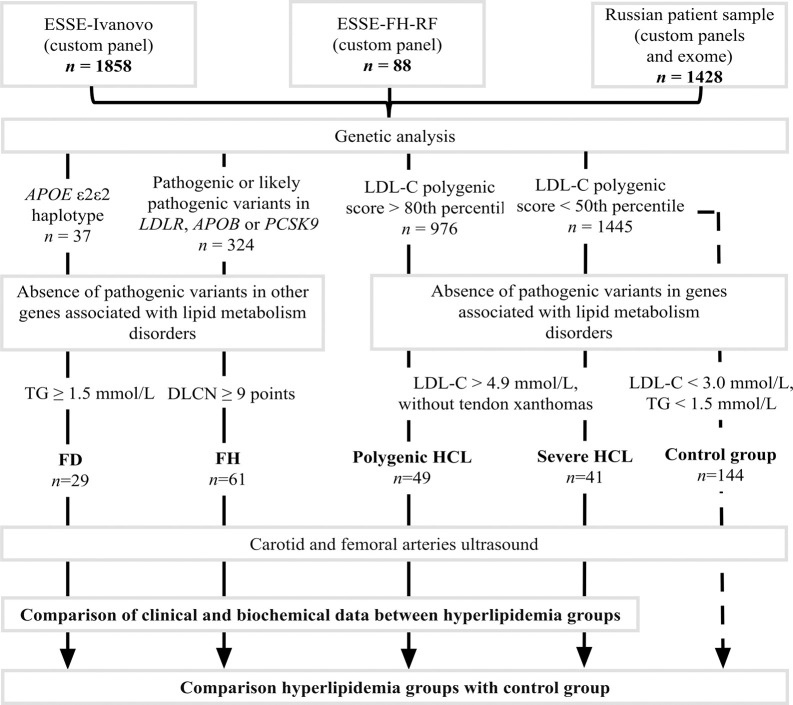
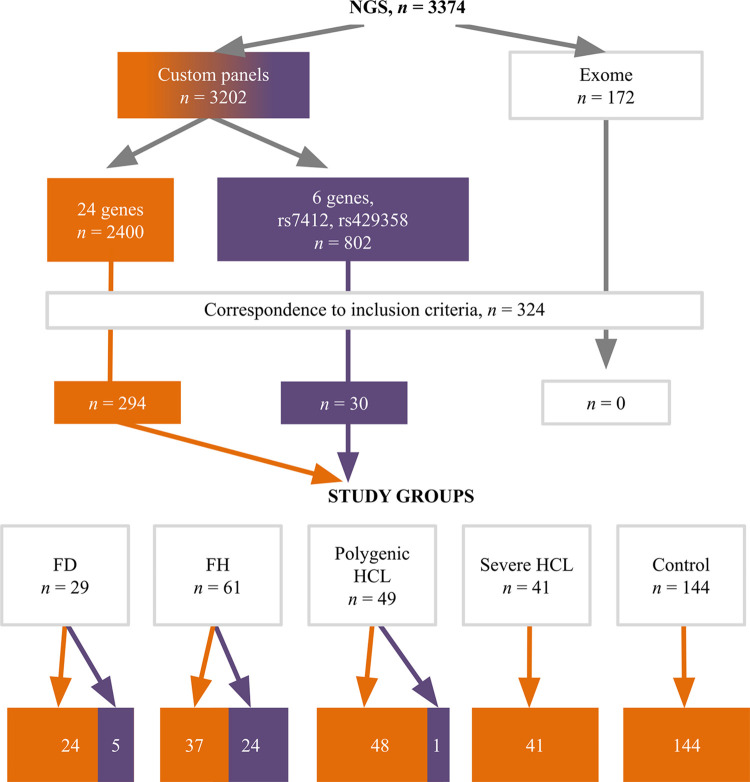
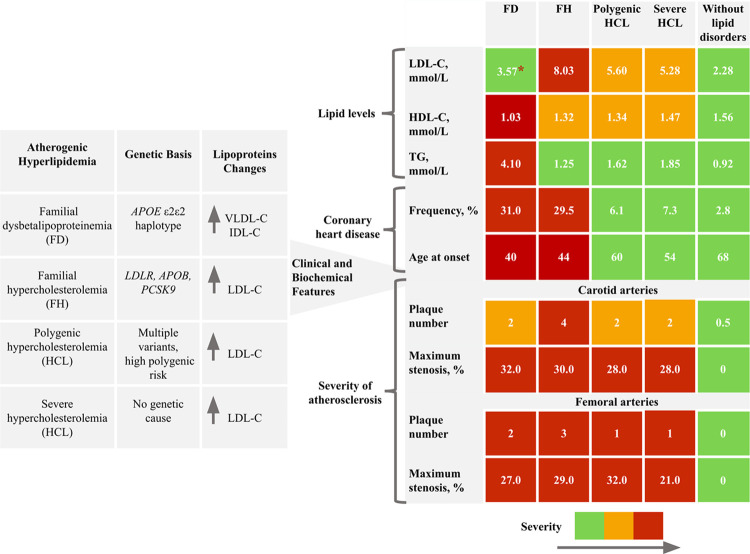
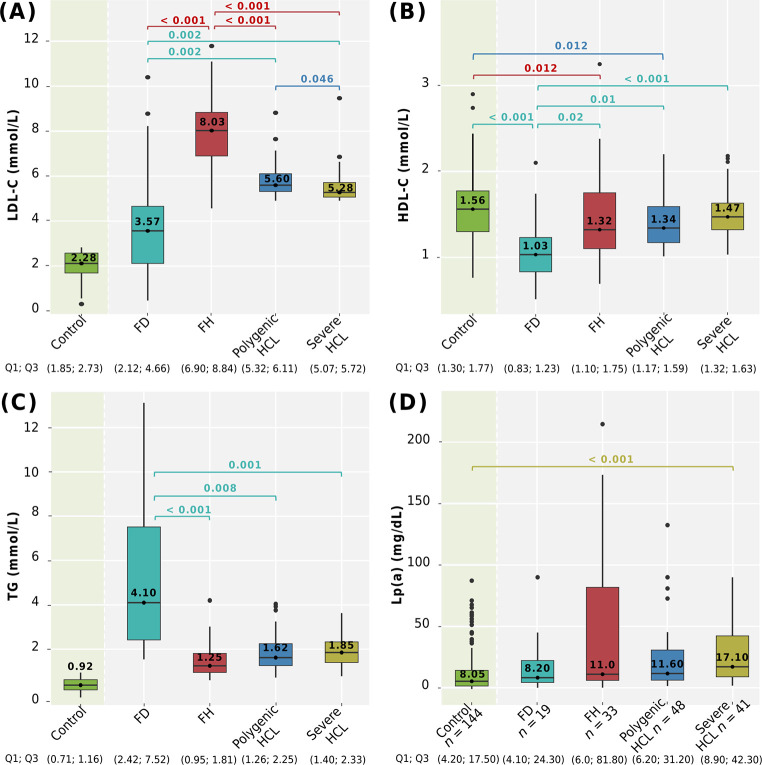
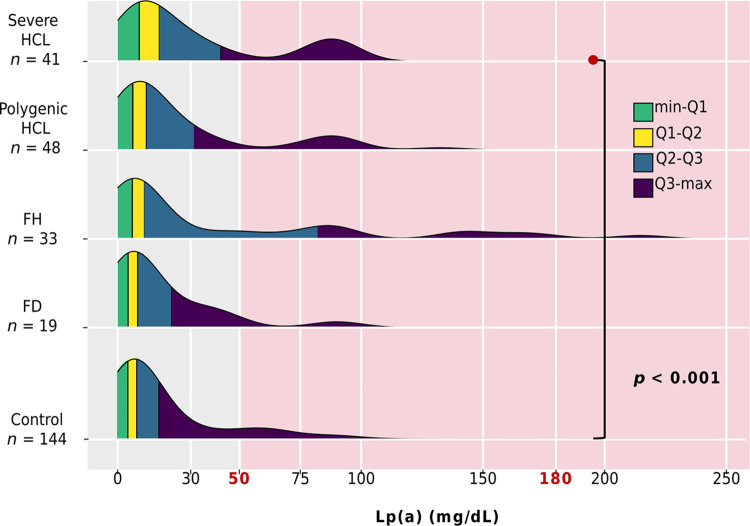
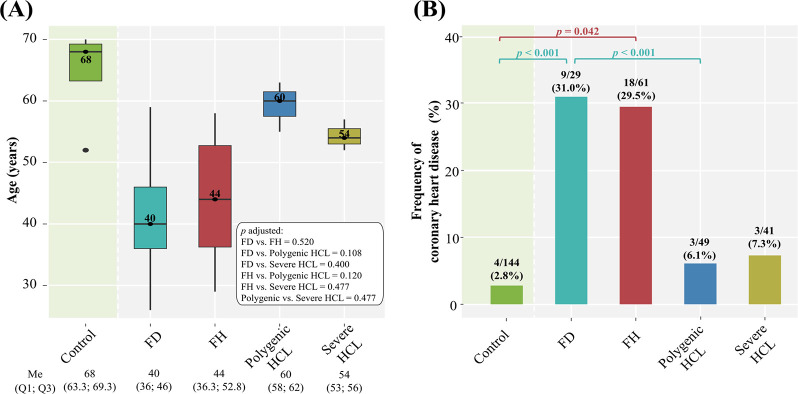
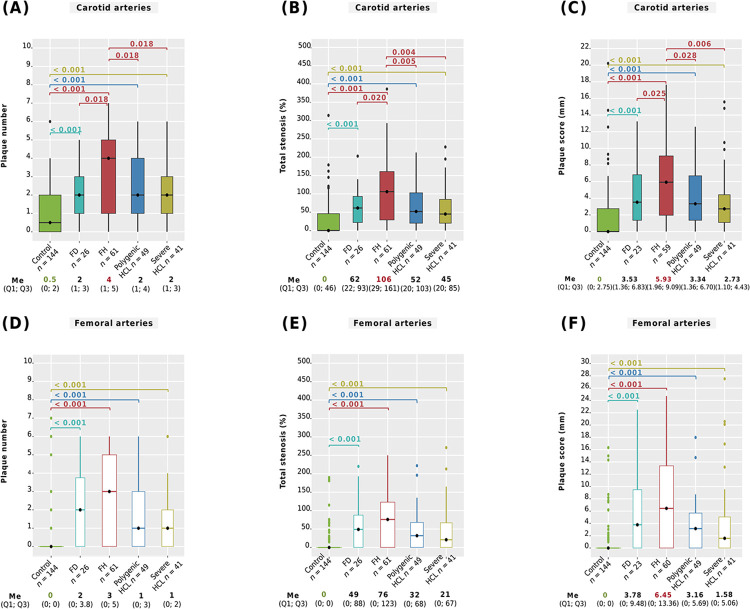
Patients with genetically-based hyperlipidemias exhibit a wide phenotypic variability. Investigation of clinical and biochemical features is important for identifying genetically-based hyperlipidemias, determining disease prognosis, and initiating timely treatment. We analyzed genetic data from 3374 samples and compared clinical data, lipid levels (low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol, triglycerides, and lipoprotein (a)), frequency, age at onset of coronary heart disease (CHD), and the severity of carotid and femoral atherosclerosis (plaque number, maximum stenosis, total stenosis, maximum plaque height, and plaque score) among patients with familial hypercholesterolemia (FH), familial dysbetalipoproteinemia (FD), polygenic hypercholesterolemia (HCL), severe HCL, and those without lipid disorders (n = 324). FH patients exhibited the highest LDL-C (median 8.03 mmol/L, p < 0.001). FD patients had elevated triglyceride levels (median 4.10 mmol/L), lower LDL-C (median 3.57 mmol/L), and high-density lipoprotein cholesterol (median 1.03 mmol/L) compared to FH, polygenic HCL, and severe HCL, p < 0.05. FH and FD patients had similar early onset of CHD, with a median age of 44 and 40 years and comparable frequencies of 29.5% and 31.0%, respectively. They were more likely to develop CHD than subjects without lipid disorders (p = 0.042 and p < 0.001, respectively). Additionally, FH patients had higher a carotid plaque number, total carotid stenosis, and carotid plaque score. This study presents the first simultaneous comparison of clinical and biochemical features among FD, FH, polygenic, and severe HCL, along with the first comprehensive evaluation of carotid and femoral atherosclerosis ultrasound parameters in FD patients. The results highlight distinct phenotypic features unique to each hyperlipidemia analyzed and underscore FH and FD as the most atherogenic hyperlipidemias.
Copyright: © 2024 Blokhina et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Beyond early LDL cholesterol lowering to prevent coronary atherosclerosis in familial hypercholesterolaemia.Eur J Prev Cardiol. 2024 May 11;31(7):892-900. doi: 10.1093/eurjpc/zwae028. Eur J Prev Cardiol. 2024. PMID: 38243822
-
Familial hypercholesterolemia: molecular, biochemical, and clinical characterization of a French-Canadian pediatric population.Pediatrics. 1995 Aug;96(2 Pt 1):239-46. Pediatrics. 1995. PMID: 7630677
-
Lipoprotein-associated phospholipase A₂ activity is increased in patients with definite familial hypercholesterolemia compared with other forms of hypercholesterolemia.Nutr Metab Cardiovasc Dis. 2018 May;28(5):517-523. doi: 10.1016/j.numecd.2018.01.012. Epub 2018 Feb 2. Nutr Metab Cardiovasc Dis. 2018. PMID: 29525223
-
The molecular genetic basis and diagnosis of familial hypercholesterolemia in Denmark.Dan Med Bull. 2002 Nov;49(4):318-45. Dan Med Bull. 2002. PMID: 12553167 Review.
-
Guidelines for the detection of high-risk lipoprotein profiles and the treatment of dyslipoproteinemias. Canadian Lipoprotein Conference Ad Hoc Committee on Guidelines for Dyslipoproteinemias.CMAJ. 1990 Jun 15;142(12):1371-82. CMAJ. 1990. PMID: 2190685 Free PMC article. Review.
Cited by
-
Genetic and Metabolic Factors of Familial Dysbetalipoproteinemia Phenotype: Insights from a Cross-Sectional Study.Int J Mol Sci. 2025 Jul 30;26(15):7376. doi: 10.3390/ijms26157376. Int J Mol Sci. 2025. PMID: 40806502 Free PMC article.
References
-
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al.. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J. 2020; 41:111–188. doi: 10.1093/eurheartj/ehz455 - DOI - PubMed
-
- Hu P, Dharmayat KI, Stevens CA, Sharabiani MT, Jones RS, Watts GF, et al.. Prevalence of familial hypercholesterolemia among the general population and patients with atherosclerotic cardiovascular disease: a systematic review and meta-analysis. Circulation. 2020; 141:1742–1759. doi: 10.1161/CIRCULATIONAHA.119.044795 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
