

Transcatheter tricuspid valve intervention versus medical therapy for symptomatic tricuspid regurgitation: a meta-analysis of reconstructed time-to-event data
- PMID: 39705669
- PMCID: PMC11487027
- DOI: 10.1097/JS9.0000000000001773
Transcatheter tricuspid valve intervention versus medical therapy for symptomatic tricuspid regurgitation: a meta-analysis of reconstructed time-to-event data
Abstract
Background: Transcatheter tricuspid valve intervention (TTVI) has demonstrated safety and efficacy in treating high-risk patients with tricuspid regurgitation (TR). The authors aimed to perform a meta-analysis based on reconstructed time-to-event data to compare the clinical benefit of TTVI with medical therapy (MED).
Methods: A systematic literature search was conducted in major databases, including PubMed, Embase, and the Cochrane Library, until 20 October 2023. All studies comparing the outcomes between TTVI and MED were included. The primary outcome was all-cause mortality. The secondary outcomes included heart failure (HF) hospitalization and the composite outcome of all-cause mortality and HF hospitalization.
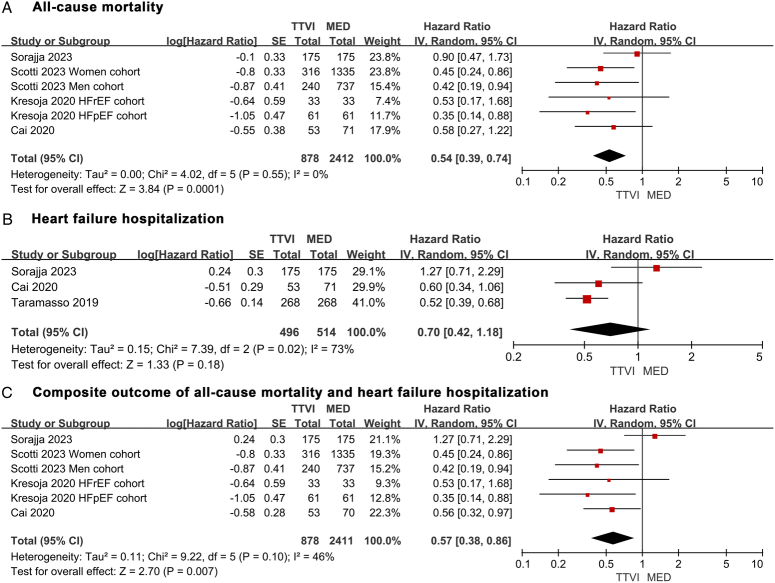
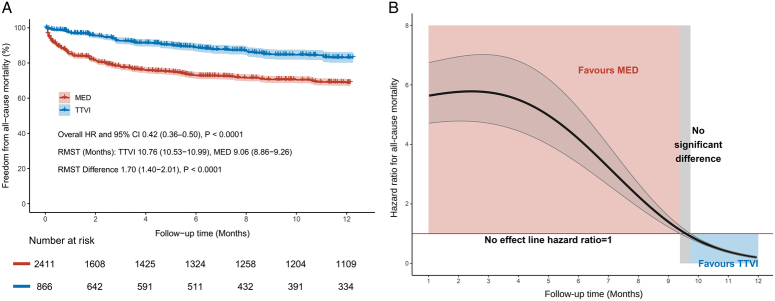
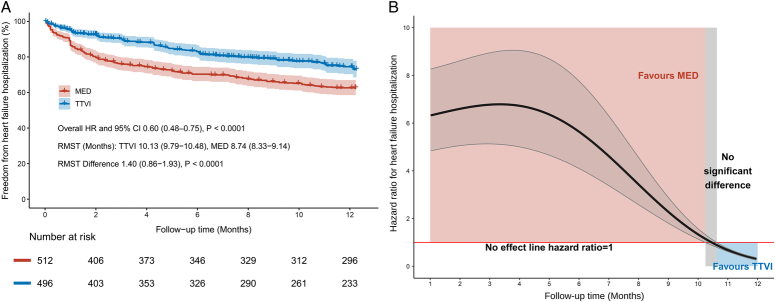
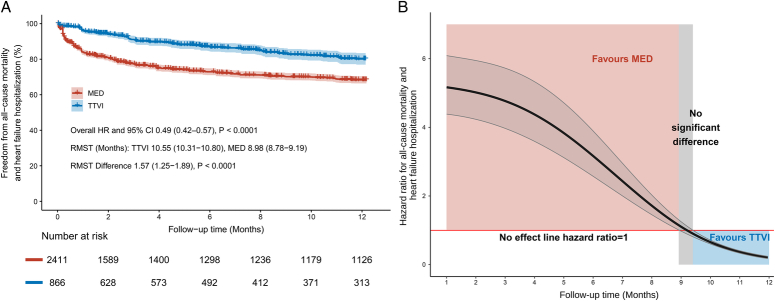
Results: Five studies covering 3826 patients (1146 received TTVI and 2680 received MED) were identified. At 1-year follow-up, TTVI significantly reduced the risk of all-cause mortality compared with MED [hazard ratio (HR) 0.54, 95% CI: 0.39-0.74, P=0.0001]. There was a trend in favor of TTVI in HF hospitalization, although without significant difference (HR 0.70, 95% CI: 0.42-1.18, P=0.18). TTVI was also associated with a decreased risk of composite outcome (HR 0.57, 95% CI: 0.38-0.86, P=0.007). Reconstructed Kaplan-Meier curves illustrated a 1-year overall survival rate of 83.1% in the TTVI group and 68.8% in the MED group. The subgroup analysis of device types yielded consistent results.
Conclusions: Compared with MED, TTVI was associated with greater 1-year benefits for patients with symptomatic moderate or greater TR from the aspects of all-cause mortality and HF hospitalization.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
All authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Impact of Massive or Torrential Tricuspid Regurgitation in Patients Undergoing Transcatheter Tricuspid Valve Intervention.JACC Cardiovasc Interv. 2020 Sep 14;13(17):1999-2009. doi: 10.1016/j.jcin.2020.05.011. JACC Cardiovasc Interv. 2020. PMID: 32912460
-
Sex-related characteristics and short-term outcomes of patients undergoing transcatheter tricuspid valve intervention for tricuspid regurgitation.Eur Heart J. 2023 Mar 7;44(10):822-832. doi: 10.1093/eurheartj/ehac735. Eur Heart J. 2023. PMID: 36445158
-
Burden of Heart Failure in Patients With Tricuspid Regurgitation and Effect of Transcatheter Repair on Different Subdimensions of Quality of Life.J Am Heart Assoc. 2024 Aug 20;13(16):e034112. doi: 10.1161/JAHA.124.034112. Epub 2024 Aug 13. J Am Heart Assoc. 2024. PMID: 39136306 Free PMC article.
-
Comparing Transcatheter Tricuspid Valve Intervention With Medical and Surgical Management: A Systematic Review and Meta-Analysis.Cureus. 2025 Apr 28;17(4):e83105. doi: 10.7759/cureus.83105. eCollection 2025 Apr. Cureus. 2025. PMID: 40438822 Free PMC article. Review.
-
Transcatheter Interventions for Tricuspid Valve Disease: What to Do and Who to Do It On.Can J Cardiol. 2021 Jul;37(7):953-967. doi: 10.1016/j.cjca.2020.12.029. Epub 2021 Jan 22. Can J Cardiol. 2021. PMID: 33493660 Review.
Cited by
-
The expression profiles and roles of microRNAs in cardiac glucose metabolism.Front Endocrinol (Lausanne). 2025 Jul 23;16:1565385. doi: 10.3389/fendo.2025.1565385. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40771283 Free PMC article.
References
-
- Topilsky Y, Maltais S, Medina Inojosa J, et al. . Burden of tricuspid regurgitation in patients diagnosed in the community setting. JACC Cardiovasc Imaging 2019;12:433–442. - PubMed
-
- Russo G, Taramasso M, Pedicino D, et al. . Challenges and future perspectives of transcatheter tricuspid valve interventions: adopt old strategies or adapt to new opportunities? Eur J Heart Fail 2022;24:442–454. - PubMed
-
- Chorin E, Rozenbaum Z, Topilsky Y, et al. . Tricuspid regurgitation and long-term clinical outcomes. Eur Heart J Cardiovasc Imaging 2020;21:157–165. - PubMed
-
- Enriquez-Sarano M, Messika-Zeitoun D, Topilsky Y, et al. . Tricuspid regurgitation is a public health crisis. Prog Cardiovasc Dis 2019;62:447–451. - PubMed
-
- Hahn RT, Lawlor MK, Davidson CJ, et al. . Tricuspid valve academic research consortium definitions for tricuspid regurgitation and trial endpoints. J Am Coll Cardiol 2023;82:1711–1735. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
