

Feature-interactive Siamese graph encoder-based image analysis to predict STAS from histopathology images in lung cancer
- PMID: 39706875
- PMCID: PMC11662006
- DOI: 10.1038/s41698-024-00771-y
Feature-interactive Siamese graph encoder-based image analysis to predict STAS from histopathology images in lung cancer
Abstract
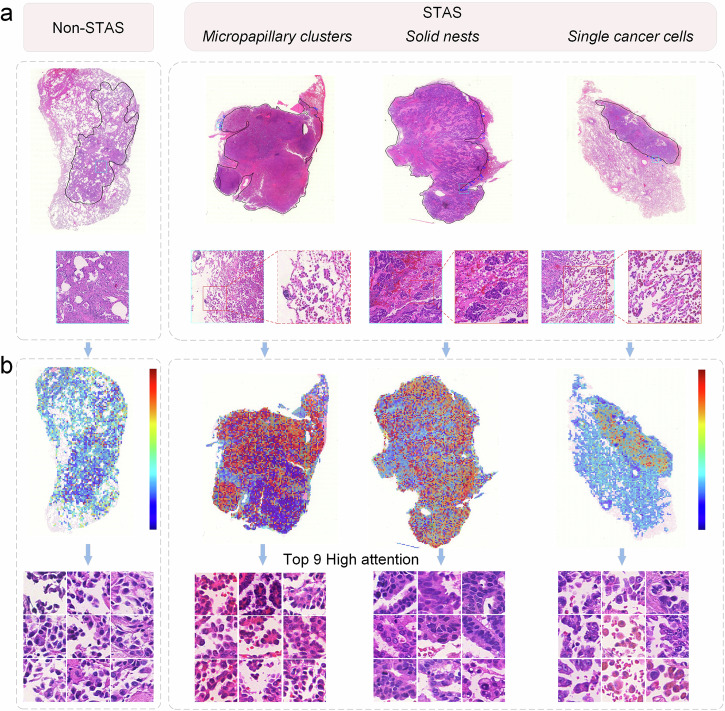
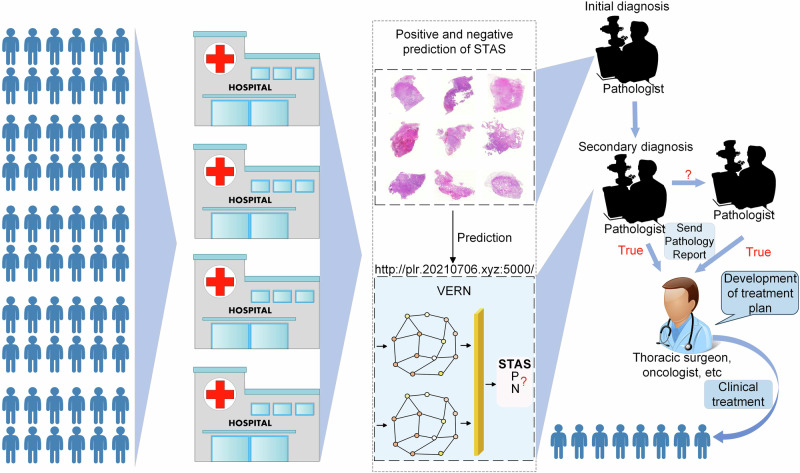
Spread through air spaces (STAS) is a distinct invasion pattern in lung cancer, crucial for prognosis assessment and guiding surgical decisions. Histopathology is the gold standard for STAS detection, yet traditional methods are subjective, time-consuming, and prone to misdiagnosis, limiting large-scale applications. We present VERN, an image analysis model utilizing a feature-interactive Siamese graph encoder to predict STAS from lung cancer histopathological images. VERN captures spatial topological features with feature sharing and skip connections to enhance model training. Using 1,546 histopathology slides, we built a large single-cohort STAS lung cancer dataset. VERN achieved an AUC of 0.9215 in internal validation and AUCs of 0.8275 and 0.8829 in frozen and paraffin-embedded test sections, respectively, demonstrating clinical-grade performance. Validated on a single-cohort and three external datasets, VERN showed robust predictive performance and generalizability, providing an open platform ( http://plr.20210706.xyz:5000/ ) to enhance STAS diagnosis efficiency and accuracy.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
LinkOut - more resources
Full Text Sources
