

Intermittent theta burst stimulation vs. high-frequency repetitive transcranial magnetic stimulation for post-stroke dysfunction: a Bayesian model-based network meta-analysis of RCTs
- PMID: 39707110
- PMCID: PMC11919949
- DOI: 10.1007/s10072-024-07918-6
Intermittent theta burst stimulation vs. high-frequency repetitive transcranial magnetic stimulation for post-stroke dysfunction: a Bayesian model-based network meta-analysis of RCTs
Abstract
Objective: This research aims to comprehensively assess the efficacy of intermittent theta-burst stimulation (iTBS) vs. high-frequency repetitive transcranial magnetic stimulation (HF-rTMS) in post-stroke dysfunction.
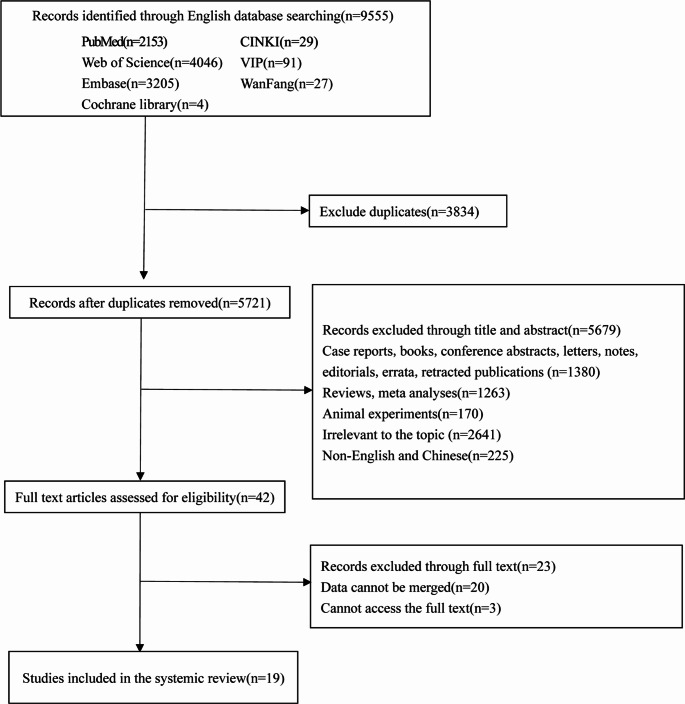
Materials and methods: Until January 2024, extensive electronic database searches were conducted (PubMed, Embase, Cochrane Library, Web of Science, etc.). Fugl-Meyer Assessment for Upper Extremities (FMA-UE) was used to assess upper limb (UL) dysfunction; post-stroke dysphagia (PSD) was identified by Standardized Swallowing Assessment (SSA), Fiberoptic Endoscopic Dysphagia Severity Scale (FEDSS), and Penetration/Aspiration Scale (PAS). Results were analyzed by network meta-analysis (NMA), and the mean difference (MD) and 95% confidence intervals (95% CI) were also reported. We conducted a descriptive analysis due to the inability to synthesize data on post-stroke cognitive impairment (PSCI).
Results: 19 studies were included for NMA analysis. For UL disorder, the efficacy of treatments was ranked as HF-rTMS [MD (95%CI):3.00 (1.69,4.31)], iTBS [MD (95%CI): 2.16 (0.84, 3.50)], and sham stimulation (reference). For PSD, the efficacy of treatment to reduce scores of FEDSS or SSA were iTBS [FEDSS, MD (95%CI): -0.80 (-1.13, -0.47); SSA, MD (95%CI): -3.37 (-4.36, -2.38)], HF-rTMS [FEDSS, MD (95%CI): -0.43 (-0.76, -0.10); SSA, MD (95%CI): -2.62 (-3.91, -1.35)], and sham stimulation(reference). Descriptive analysis of PSCI found that both iTBS and HF-rTMS were effective in improving PSCI.
Conclusions: HF-rTMS demonstrates superior efficacy in UL dysfunction, while iTBS is more effective in PSD. Clinicians should carefully evaluate the type and severity of post-stroke dysfunction in each patient to select the most appropriate treatment.
Keywords: HF-rTMS; Network meta-analysis; Post-stroke dysfunction; iTBS.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable, our study is based on open-source public database, and the Quanzhou First Hospital Affiliated to Fujian Medical University do not require research using publicly available data to be submitted for review to their ethics committee, so there are no ethical issues and other conflicts of interest. Consent for publication: Not applicable. Conflict of interest: All authors declare that they have no conflict of interests.
Figures


Similar articles
-
Bilateral Cerebellar Intermittent Theta Burst Stimulation Combined With Swallowing Speech Therapy for Dysphagia After Stroke: A Randomized, Double-Blind, Sham-Controlled, Clinical Trial.Neurorehabil Neural Repair. 2022 Jul;36(7):437-448. doi: 10.1177/15459683221092995. Epub 2022 May 16. Neurorehabil Neural Repair. 2022. PMID: 35574927 Clinical Trial.
-
Effectiveness of intermittent theta burst stimulation (iTBS) for managing post-stroke dysphagia: systematic review and meta-analysis.Top Stroke Rehabil. 2025 Sep;32(6):652-661. doi: 10.1080/10749357.2024.2437325. Epub 2024 Dec 8. Top Stroke Rehabil. 2025. PMID: 39647505 Review.
-
Comparative Efficacy of Different Repetitive Transcranial Magnetic Stimulation Protocols for Stroke: A Network Meta-Analysis.Front Neurol. 2022 Jun 15;13:918786. doi: 10.3389/fneur.2022.918786. eCollection 2022. Front Neurol. 2022. PMID: 35785350 Free PMC article.
-
Effects of Cerebellar Repetitive Transcranial Magnetic Stimulation in the Treatment of Post-Stroke Dysphagia: A Meta-Analysis and Systematic Review of Randomized Controlled Trials.Eur Neurol. 2024;87(2):67-78. doi: 10.1159/000538130. Epub 2024 Mar 2. Eur Neurol. 2024. PMID: 38432194
-
Theta-burst transcranial magnetic stimulation for dysphagia patients during recovery stage of stroke: a randomized controlled trial.Eur J Phys Rehabil Med. 2023 Oct;59(5):543-553. doi: 10.23736/S1973-9087.23.08023-1. Epub 2023 Sep 22. Eur J Phys Rehabil Med. 2023. PMID: 37737051 Free PMC article. Clinical Trial.
References
-
- Feigin VL, Brainin M, Norrving B, Martins S, Sacco RL, Hacke W, Fisher M, Pandian J, Lindsay P (2022) World Stroke Organization (WSO): global stroke fact sheet 2022. Int J Stroke: Official J Int Stroke Soc 17(1):18–29. 10.1177/17474930211065917 - PubMed
-
- Kisoli A, Gray WK, Dotchin CL, Orega G, Dewhurst F, Paddick SM, Longdon A, Chaote P, Dewhurst M, Walker RW (2015) Levels of functional disability in elderly people in Tanzania with dementia, stroke and Parkinson’s disease. Acta Neuropsychiatrica 27(4):206–212. 10.1017/neu.2015.9 - PubMed
-
- Georgakis MK, Fang R, Düring M, Wollenweber FA, Bode FJ, Stösser S, Kindlein C, Hermann P, Liman TG, Nolte CH et al (2023) Cerebral small vessel disease burden and cognitive and functional outcomes after stroke: a multicenter prospective cohort study. Alzheimer’s Dement J Alzheimer’s Assoc 19(4):1152–1163. 10.1002/alz.12744 - PubMed
-
- Langhorne P, Coupar F, Pollock A (2009) Motor recovery after stroke: a systematic review. Lancet Neurol 8(8):741–754. 10.1016/s1474-4422(09)70150-4 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
