

Efficacy and safety of neoadjuvant S-1-based chemoradiotherapy in resectable and borderline-resectable pancreatic cancer: a long-term follow-up study
- PMID: 39707428
- PMCID: PMC11662451
- DOI: 10.1186/s12957-024-03609-w
Efficacy and safety of neoadjuvant S-1-based chemoradiotherapy in resectable and borderline-resectable pancreatic cancer: a long-term follow-up study
Abstract
Background/objectives: This study aimed to evaluate the safety, efficacy, and long-term outcomes of S-1-based neoadjuvant chemoradiotherapy (NACRT) in patients with resectable or borderline-resectable pancreatic ductal adenocarcinoma (PDAC).
Methods: This retrospective study included patients with PDAC who underwent S-1-based NACRT at our institute between 2010 and 2017.
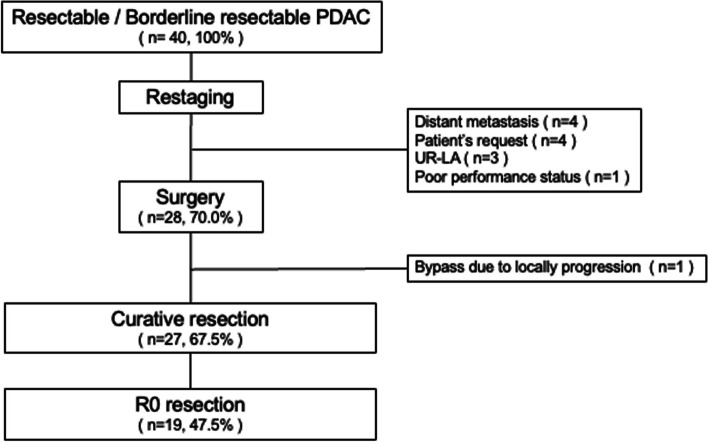
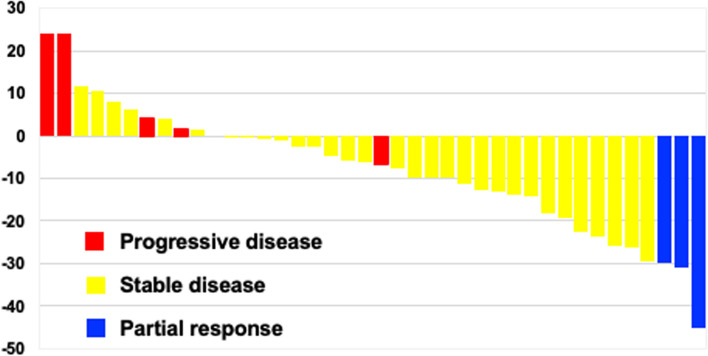
Results: Forty patients were included in the study, including 15 (37.5%) with resectable PDAC and 25 (62.5%) with borderline-resectable PDAC. The NACRT completion and resection rates were 85.0% (n = 34) and 67.5% (n = 27), respectively. Several grade 3 adverse events were observed, including leukopenia (25.0%), anorexia (17.5%), neutropenia (10.0%), thrombocytopenia (7.5%), febrile neutropenia (2.5%), elevated aspartate aminotransferase/alanine aminotransferase (2.5%) levels, and hyponatremia (2.5%). The R0 resection rate was 70.4% (n = 19/27) in patients who underwent pancreatectomy. Grades 1, 2, and 3 according to the College of American Pathologists grading system were observed in 1 (3.7%), 12 (44.4%), and 14 (51.9%) patients, respectively. Over a median follow-up period of 32.9 months (interquartile range, 9.1-68.0), the 1-, 3-, and 5-year OS rates were 81.4%, 45.5%, and 30.3%, respectively, in the intention-to-treat analysis. In the curative-intent surgery cohort (n = 27), the 1-, 3-, and 5-year OS rates were 88.9%, 48.2%, and 37.0%, respectively.
Conclusions: S-1-based NACRT is safe and yields acceptable long-term outcomes for patients with resectable or borderline-resectable PDAC.
Keywords: Pancreatic ductal adenocarcinoma; Resection; Retrospective study; S-1-based neoadjuvant chemoradiotherapy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study design was approved by the Institutional Review Board of Keio University School of Medicine (#20090127). Informed consent was obtained from all individual participants included in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Hori M, Matsuda T, Shibata A, Katanoda K, Sobue T, Nishimoto H, et al. Cancer incidence and incidence rates in Japan in 2009: a study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol. 2015;45:884–91. 10.1093/jjco/hyv088. - DOI - PubMed
-
- Jang J, Han Y, Lee H, Kim S, Kwon W, Lee K, et al. Oncological benefits of neoadjuvant chemoradiation with gemcitabine versus upfront surgery in patients with borderline resectable pancreatic cancer: a prospective, randomized, open-label, multicenter phase 2/3 trial. Ann Surg. 2018;268:215–22. 10.1097/SLA.0000000000002705. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
