

Polyarteritis nodosa presenting with severe upper gastrointestinal bleeding: a case report
- PMID: 39707462
- PMCID: PMC11662699
- DOI: 10.1186/s13256-024-04892-7
Polyarteritis nodosa presenting with severe upper gastrointestinal bleeding: a case report
Abstract
Background: Polyarteritis nodosa is a relatively uncommon type of systemic necrotizing vasculitis that primarily affects medium-sized arteries. While gastrointestinal involvement is known in polyarteritis nodosa, heavy gastrointestinal bleeding due to gastric ulceration is relatively uncommon. We present the case of an 81-year-old male of Chinese ethnicity who experienced severe gastrointestinal bleeding as a result of polyarteritis nodosa and an innovative treatment approach for a better patient outcomes.
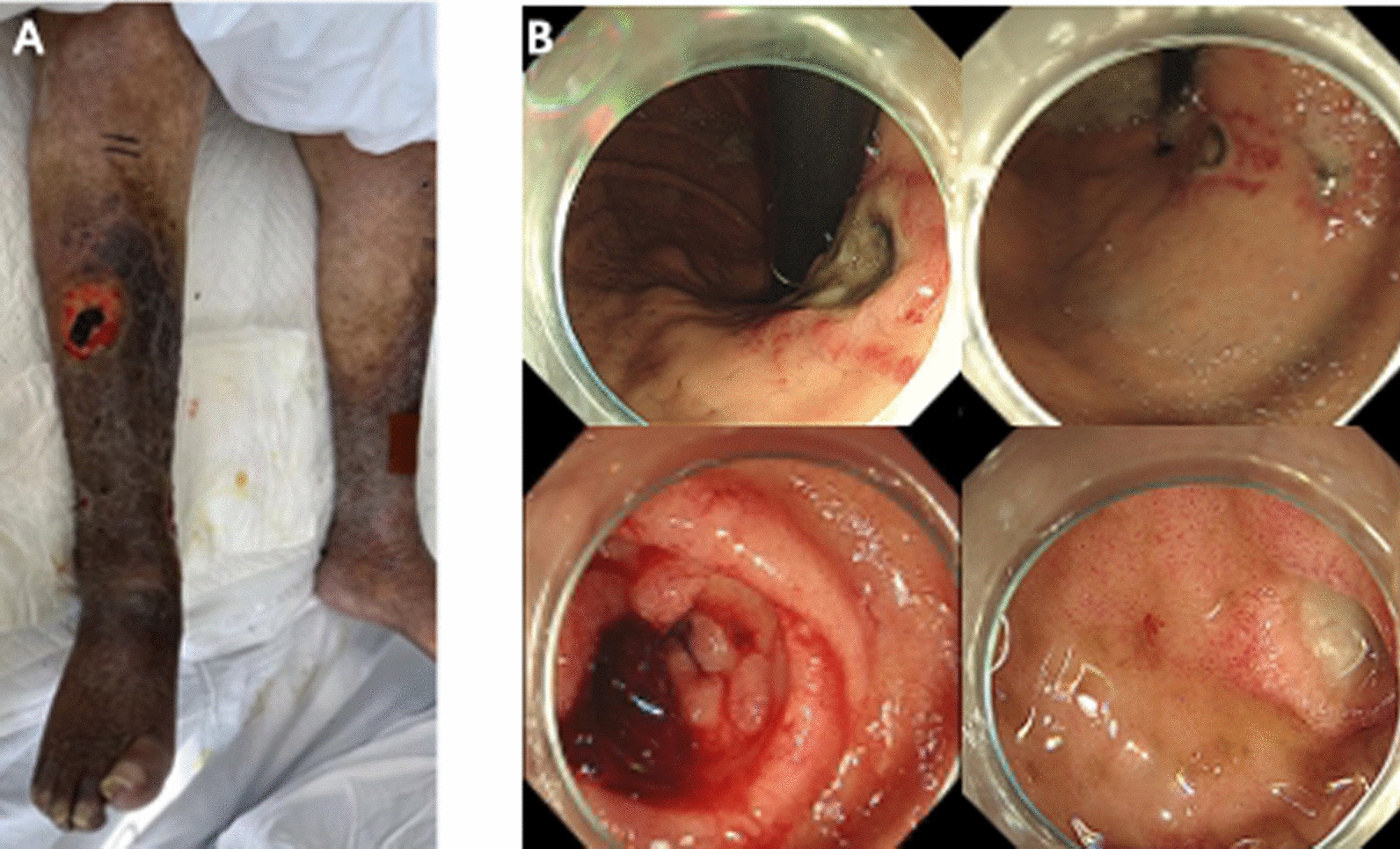
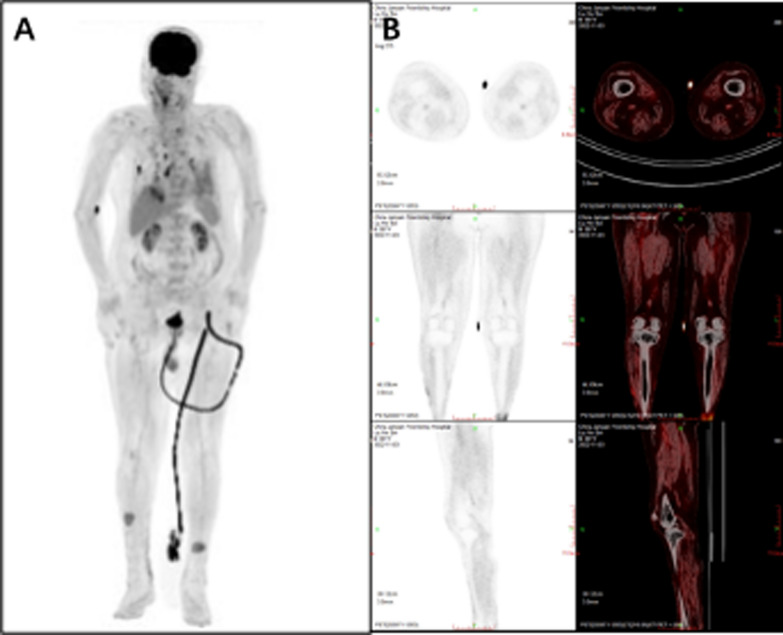
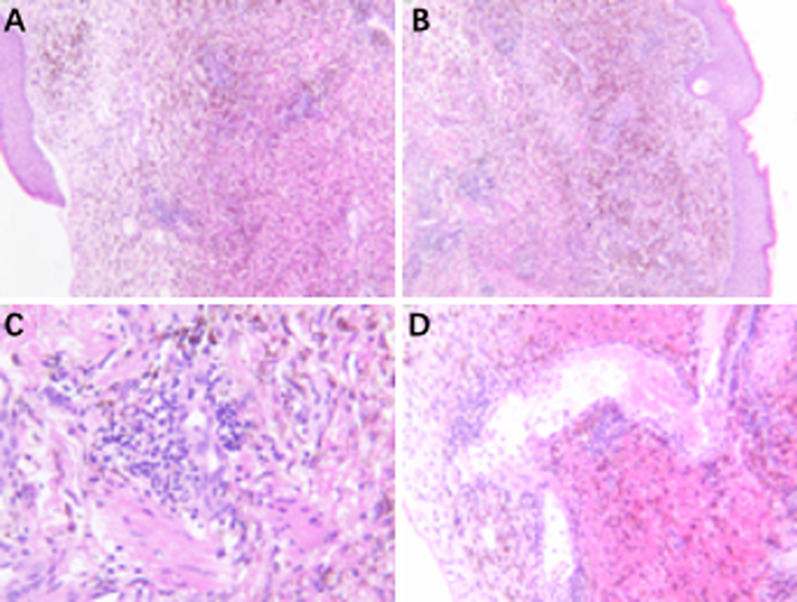
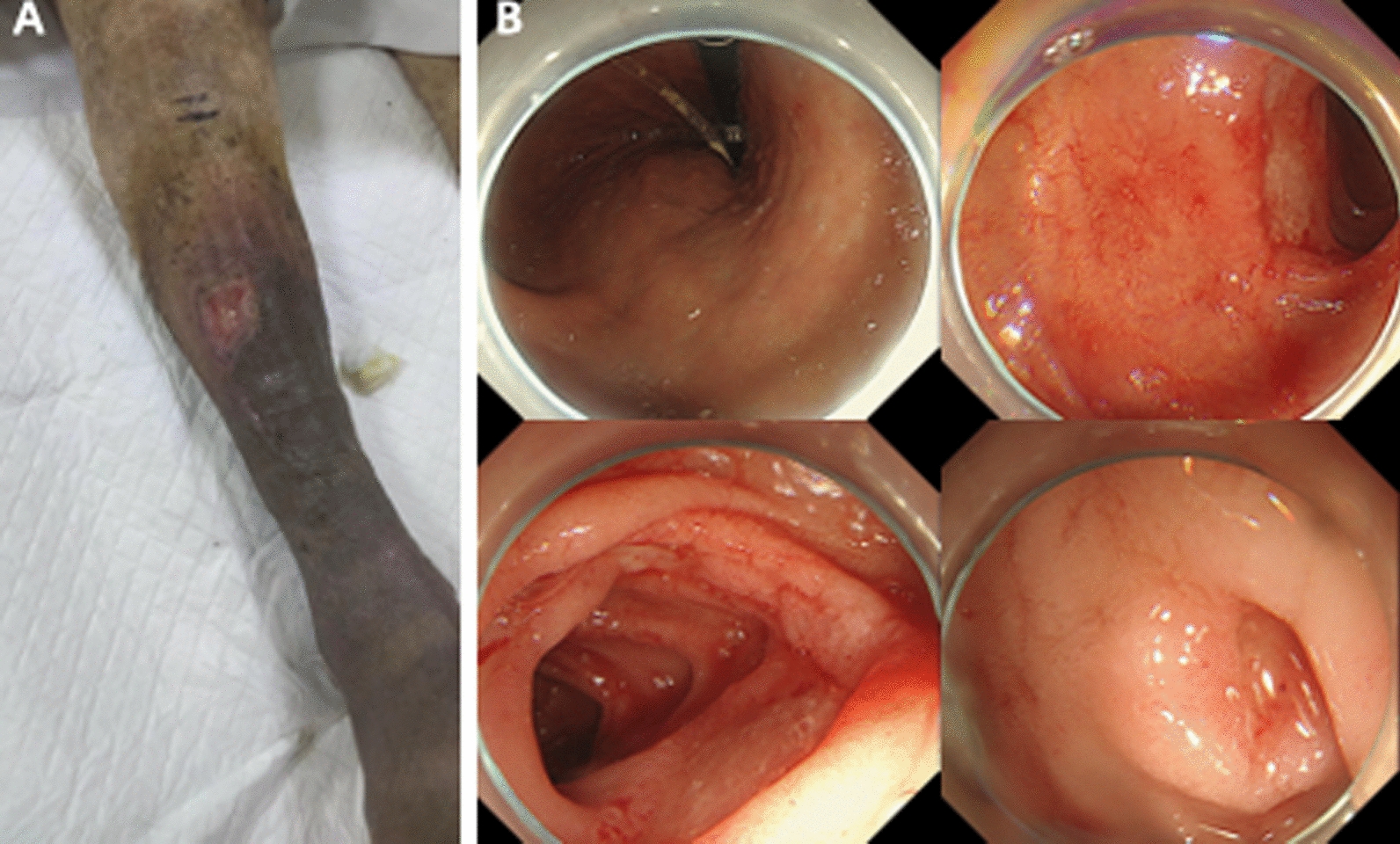
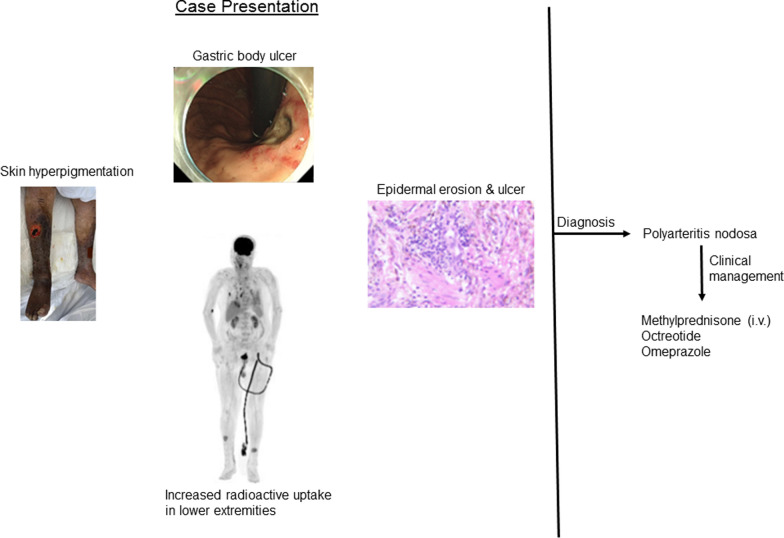
Case presentation: Upon admission to the medical intensive care unit, the patient underwent a comprehensive diagnostic assessment, including examinations for cardiovascular and dermatological abnormalities, laboratory tests, autoantibody and tumor marker assessments, and imaging studies (such as endoscopies, whole-body computed tomography, and positron emission tomography-computed tomography scans), and a skin biopsy. The patient had tachycardia, hypotension, and extensive skin abnormalities on the lower extremities along with anemia, low platelets, and abnormal renal function. Upper gastrointestinal endoscopy revealed gastric and duodenal ulcers. Additional examinations, including electronic colonoscopy, capsule endoscopy, and whole-body computed tomography, were negative. A positron emission tomography-computed tomography scan showed increased uptake in the arterial walls and skin, which supported the diagnosis of polyarteritis nodosa, later confirmed by a biopsy of the skin on the lower extremities. Methylprednisolone, octreotide, and omeprazole were administered, leading to improvement in gastrointestinal symptoms, ulcer healing, and skin recovery. The patient continued with prednisone for 1 month.
Conclusion: This case serves to inform gastroenterologists about the need to consider polyarteritis nodosa in severe upper gastrointestinal bleeding and underscores the importance of prompt, medication-based treatment for successful patient outcome.
Keywords: Endoscopy; Gastrointestinal bleeding; Glucocorticoid; Polyarteritis nodosa; Skin biopsy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: No IRB is required for case reports and written informed consent was obtained. Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Competing interests: Not applicable.
Figures
Similar articles
-
High incidence of Dieulafoy's lesions in upper gastrointestinal bleeding associated with polyarteritis--clinical examination of patients of polyarteritis nodosa with rapidly progressive glomerulonephritis.Hepatogastroenterology. 2008 May-Jun;55(84):821-5. Hepatogastroenterology. 2008. PMID: 18705275
-
Necrosis of the small intestine leading to a diagnosis of polyarteritis nodosa: a case report.J Med Case Rep. 2019 Mar 9;13(1):55. doi: 10.1186/s13256-019-2017-8. J Med Case Rep. 2019. PMID: 30850017 Free PMC article.
-
Polyarteritis nodosa presenting as profuse gastrointestinal bleeding.BMJ Case Rep. 2014 Feb 6;2014:bcr2013202925. doi: 10.1136/bcr-2013-202925. BMJ Case Rep. 2014. PMID: 24503664 Free PMC article.
-
Uncommon presentations of primary systemic necrotizing vasculitides: the Great Masquerades.Int J Rheum Dis. 2014 Jun;17(5):562-72. doi: 10.1111/1756-185X.12223. Epub 2013 Nov 14. Int J Rheum Dis. 2014. PMID: 24237487 Review.
-
Possible usefulness of fluorodeoxyglucose positron emission tomography in diagnosing polyarteritis nodosa: A case report and literature review.Mod Rheumatol Case Rep. 2025 Jan 16;9(1):137-142. doi: 10.1093/mrcr/rxae044. Mod Rheumatol Case Rep. 2025. PMID: 39126149 Review.
References
-
- Stone JH. Polyarteritis nodosa. JAMA. 2002;288(13):1632–9. 10.1001/jama.288.13.1632. - PubMed
-
- Rohmer J, Nguyen Y, Trefond L, et al. Clinical features and long-term outcomes of patients with systemic polyarteritis nodosa diagnosed since 2005: data from 196 patients. J Autoimmun. 2023;139: 103093. 10.1016/j.jaut.2023.103093. - PubMed
-
- Travers RL, Allison DJ, Brettle RP, et al. Polyarteritis nodosa: a clinical and angiographic analysis of 17 cases. Semin Arthritis Rheum. 1979;8(3):184–99. 10.1016/s0049-0172(79)80007-4. - PubMed
-
- Ahn E, Luk A, Chetty R, et al. Vasculitides of the gastrointestinal tract. Semin Diagn Pathol. 2009;26(2):77–88. 10.1053/j.semdp.2009.06.001. - PubMed
-
- Ebert EC, Hagspiel KD, Nagar M, et al. Gastrointestinal involvement in polyarteritis nodosa. Clin Gastroenterol Hepatol. 2008;6(9):960–6. 10.1016/j.cgh.2008.04.004. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
