

Ecteinascidin synthetic analogues: a new class of selective inhibitors of transcription, exerting immunogenic cell death in refractory malignant pleural mesothelioma
- PMID: 39709435
- PMCID: PMC11662834
- DOI: 10.1186/s13046-024-03253-y
Ecteinascidin synthetic analogues: a new class of selective inhibitors of transcription, exerting immunogenic cell death in refractory malignant pleural mesothelioma
Abstract
Background: Malignant pleural mesothelioma (MPM) is a highly chemo-refractory and immune-evasive tumor that presents a median overall survival of 12-14 months when treated with chemotherapy and immunotherapy. New anti-tumor therapies as well as the concomitant reactivation of immune destruction are urgently needed to treat patients with this tumor. The aim of this work is to investigate the potential effect of ecteinascidin derivatives as lurbinectedin as new first-line treatment option in MPM, alone and in combination with immunotherapy.
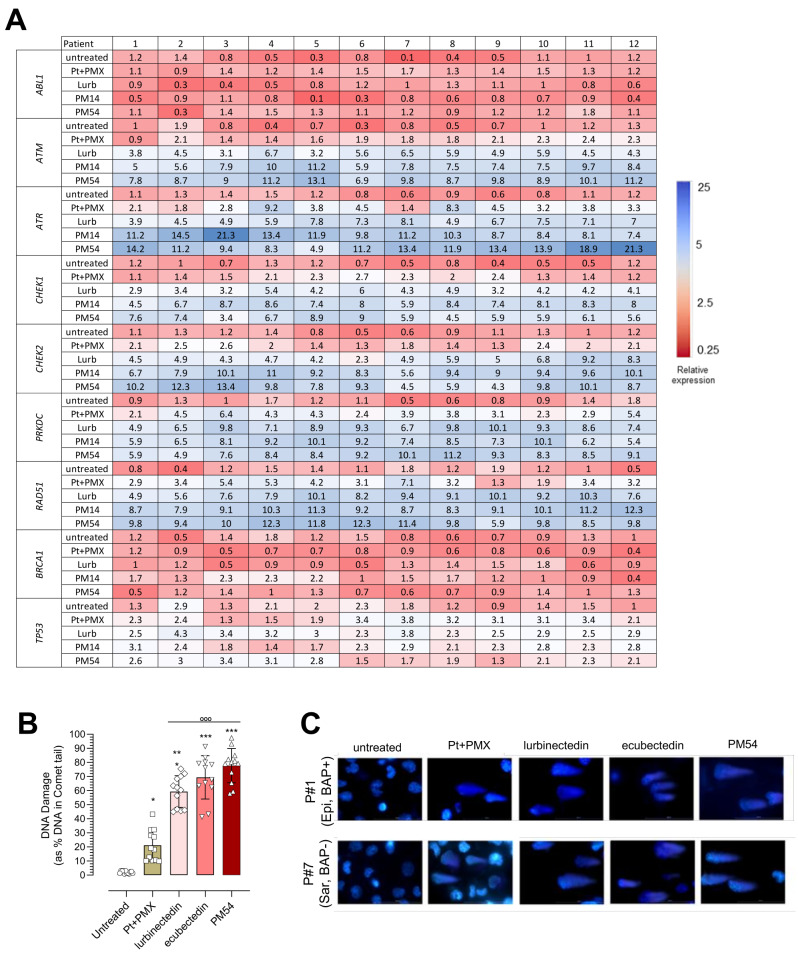
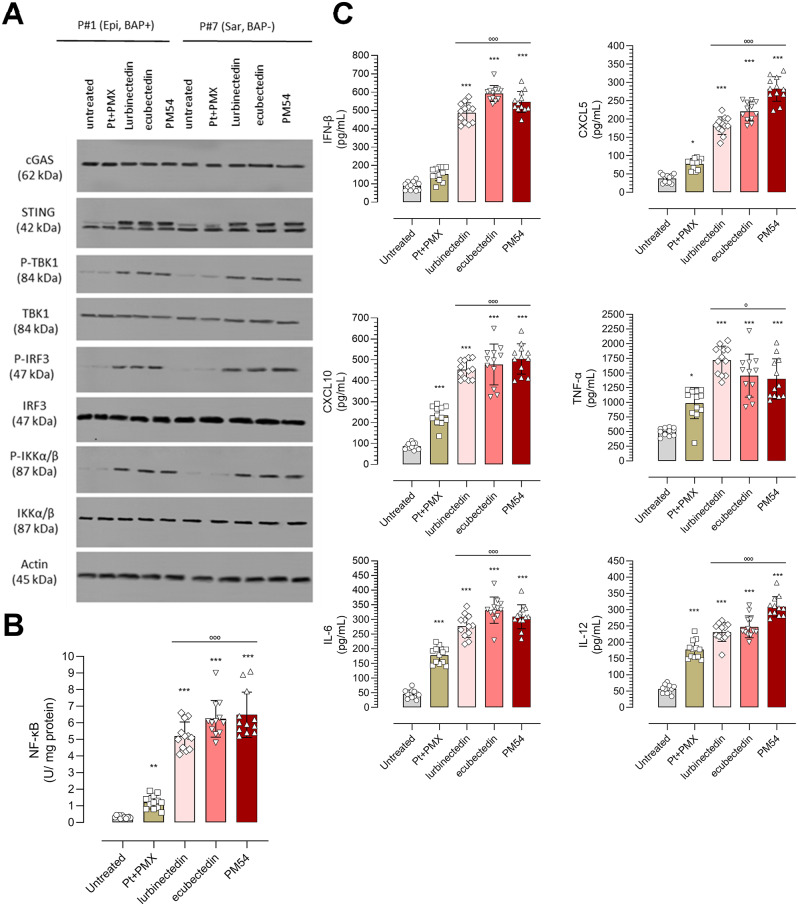
Methods: The antitumor activity of ecteinascidin synthetic analogues: lurbinectedin, ecubectedin and PM54 was evaluated in an array of patient-derived MPM cells in terms of cell proliferation, cell cycle, apoptosis, DNA damage and repair. Immunoblot was used to assess the cGAS/STING pathway. ELISA and flow cytometry-based assays were used to evaluate immunogenic cell death parameters and the effect on the immunophenotype in autologous peripheral blood monocyte-MPM cells co-cultures. Patient-derived xenografts (PDX) in humanized mice were used to evaluate the efficacy of ecteinascidins in vivo.
Results: Lurbinectedin, ecubectedin, and PM54 were effective in reducing cell proliferation and migration, as well as inducing S-phase cell cycle arrest and DNA damage in malignant pleural mesothelioma cells. These effects were more pronounced compared to the standard first-line treatment (platinum-based plus pemetrexed). Mechanistically, the drugs downregulated DNA repair genes, activated the cGAS/STING pathway, and promoted the release of pro-inflammatory cytokines. They also induced immunogenic cell death of mesothelioma cells, enhancing the activation of anti-tumor CD8+T-cells and natural killer cells while reducing tumor-tolerant T-regulatory cells and myeloid-derived suppressor cells in ex vivo co-cultures. These promising results were also observed in humanized patient-derived xenograft models, where the drugs were effective in reducing tumor growth and increasing the ratio anti-tumor/pro-tumor infiltrating immune populations, either alone or combined with the anti-PD-1L atezolizumab.
Conclusions: Collectively, these findings reveal a previously unknown mechanism of action of ecteinascidins that merits further investigation for potential clinical applications in the treatment of MPM, as new first line treatment in monotherapy or in association with immunotherapy.
Keywords: Chemo-immunotherapy; DNA damage; Ecteinascidins; Immunogenic cell death; Malignant pleural mesothelioma; cGAS/STING pathway.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the local Ethical Committee (#128/2016). The patients gave written informed consent to participate in the study. Consent for publication: The patients gave written informed consent to publish the results of the study. Competing interests: PA, HS and CC are PharmaMar S.A. employees or Pharma-Mar S.A. shareholders or both. CR received lurbinectedin and its derivatives, and economical support from PharmaMar S.A. AM received travel expense reimbursement from PharmaMar S.A. outside the present work and is member of the advisory board of Boehringer Ingelheim. LR received grants from AstraZeneca, Roche, Eli Lilly, and Novartis outside the submitted work. SN is speaker’s bureau for: Amgen, AstraZeneca, Boehringer Ingelheim, BeiGene, Eli Lilly, Pfizer, Roche, MSD, Janssen, Novartis, Takeda, Thermo Fisher, member of the advisory board and consultant for Sanofi. GVS has received grants from TESARO/GSK and personal fees as well as supports from Pfizer, AstraZeneca, Eli Lilly and MSD outside the submitted work; personal fees from Roche, Novartis, Clovis, Takeda and BeiGene outside the submitted work.
Figures



References
-
- Tagliamento M, Di Maio M, Remon J, Bironzo P, Genova C, Facchinetti F, et al. Meta-Analysis on the Combination of Chemotherapy With Programmed Death-Ligand 1 and Programmed Cell Death Protein 1 Blockade as First-Line Treatment for Unresectable Pleural Mesothelioma. J Thorac Oncol. 2024;19:166–72. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
