

Impact on fluid balance of an optimized restrictive strategy targeting non-resuscitative fluids in intensive care patients with septic shock: a single-blind, multicenter, randomized, controlled, pilot study
- PMID: 39709493
- PMCID: PMC11663312
- DOI: 10.1186/s13054-024-05155-z
Impact on fluid balance of an optimized restrictive strategy targeting non-resuscitative fluids in intensive care patients with septic shock: a single-blind, multicenter, randomized, controlled, pilot study
Abstract
Background: In septic shock, the classic fluid resuscitation strategy can lead to a potentially harmful positive fluid balance. This multicenter, randomized, single-blind, parallel, controlled pilot study assessed the effectiveness of a restrictive fluid strategy aiming to limit daily volume.
Methods: Patients 18-85 years' old admitted to the ICU department of three French hospitals were eligible for inclusion if they had septic shock and were in the first 24 h of vasopressor infusion. Exclusion criteria were acute kidney injury requiring renal replacement therapy, end stage chronic kidney disease, and severe malnutrition. Patients were electronically randomized 1:1 to either an optimized fluid restriction (reducing fluid intake as much as possible in terms of maintenance fluids and fluids for drug dilution during the first 7 days) or standard fluid strategy. The primary outcome was cumulative fluid balance (ml/kg) in the first 5 days. Patients and statisticians were blinded to group arm, but not clinicians.
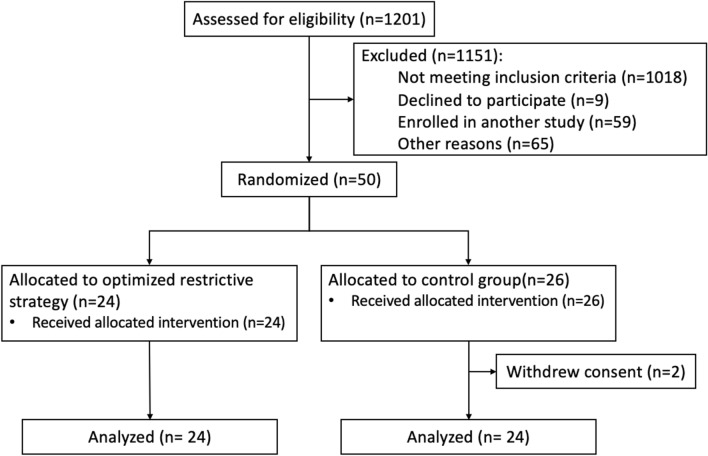
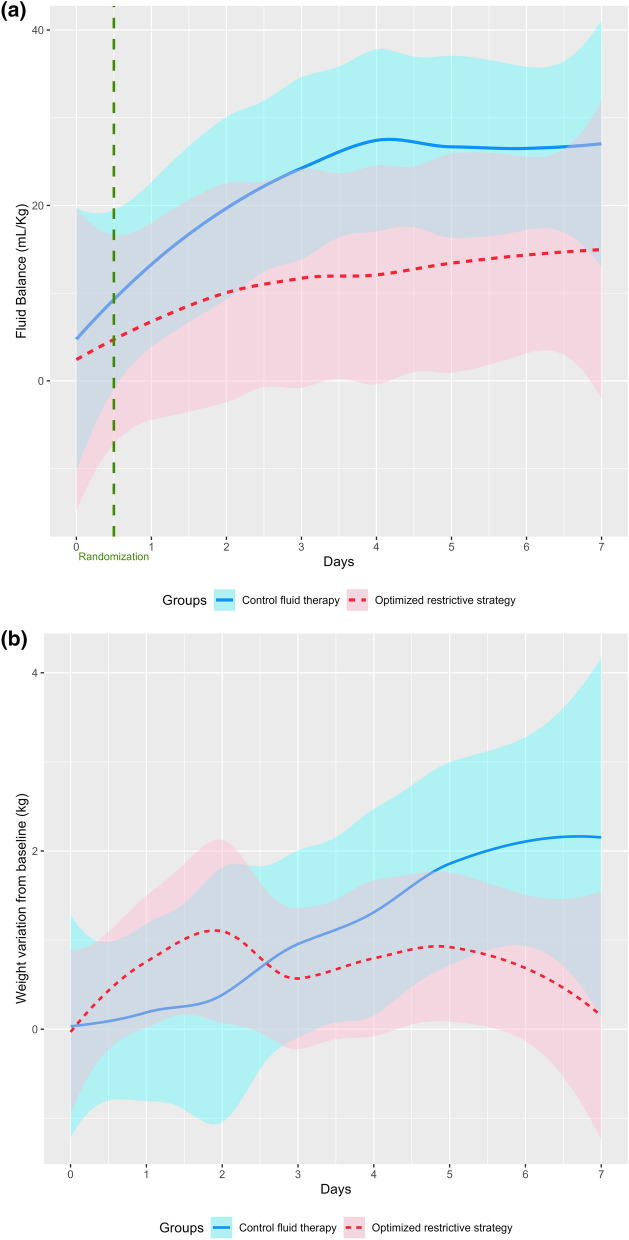
Results: Between September 2021 and February 2023, 1201 patients were screened and 50 included, with two in the control group withdrawing, thus 48 patients were analyzed (24 in each group). In the first 5 days, the optimized restrictive strategy and control groups received 89.7 (IQR 35; 128.9) and 114.3 (IQR 78.8; 168.5) ml/kg of fluid, respectively (mean difference: 35.9 ml/kg [0.0; 71.8], p = 0.0506). After 5 days, the median cumulative fluid balance was 6.9 (IQR - 13.7; 52.1) and 35.0 (IQR - 7.9; 40.2) ml/kg in the optimized restrictive strategy and control groups, respectively (absolute difference 13.2 [95%CI - 15.2; 41.6], p = 0.42). After 28 days, mortality and the numbers of days alive without life support were similar between groups. The main adverse events were severe hypernatremia in 1 and 2 patients in the fluid restriction strategy and control groups, respectively, and acute kidney injury KDIGO 3 in 4 and 7 patients in the fluid restriction strategy and control groups, respectively.
Conclusions: In ICU patients with septic shock, an optimized restrictive fluid strategy targeting hidden fluid intakes did not reduce the overall fluid balance at day 5. Trial registration ClinicalTrials.gov identifier NCT04947904, registered on 1 July 2021.
Keywords: Fluid balance; Intensive care unit; Restrictive strategy; Septic shock.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Comité de Protection des Personnes Sud-Méditerranée II (Number 2020-A01952-37). Written informed consent was obtained from patients or their legal surrogates. Consent for publication: Written informed consent was obtained from patients or their legal surrogates either before randomization or as soon as possible thereafter. Competing interests: The authors declare no competing interests.
Figures
References
-
- Heart N. Lung, and blood institute acute respiratory distress syndrome clinical trials network: comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24):2564–75. - PubMed
-
- Sakr Y, Vincent JL, Reinhart K, Groeneveld J, Michalopoulos A, Sprung CL, Artigas A, Ranieri VM. Sepsis Occurence in Acutely Ill Patients I: high tidal volume and positive fluid balance are associated with worse outcome in acute lung injury. Chest. 2005;128(5):3098–108. - PubMed
-
- Sakr Y, Rubatto Birri PN, Kotfis K, Nanchal R, Shah B, Kluge S, Schroeder ME, Marshall JC, Vincent JL. Intensive care over nations I: higher fluid balance increases the risk of death from sepsis: results from a large international audit. Crit Care Med. 2017;45(3):386–94. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
