

Pre-diagnosis and pre-treatment loss to follow-up and associated factors among patients with presumed tuberculosis and those diagnosed in Uganda
- PMID: 39710664
- PMCID: PMC11665076
- DOI: 10.1186/s12913-024-12115-4
Pre-diagnosis and pre-treatment loss to follow-up and associated factors among patients with presumed tuberculosis and those diagnosed in Uganda
Abstract
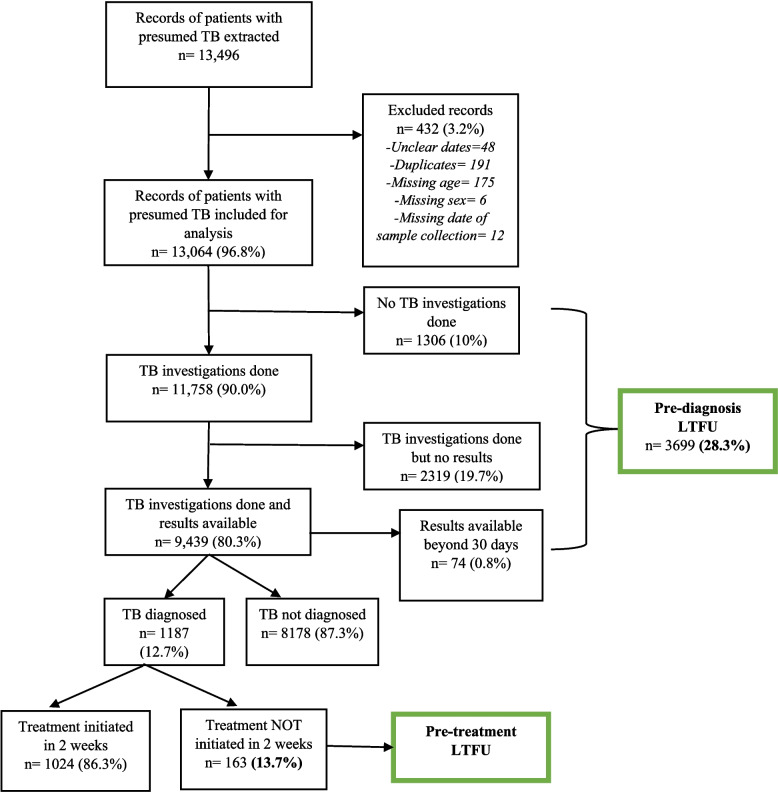
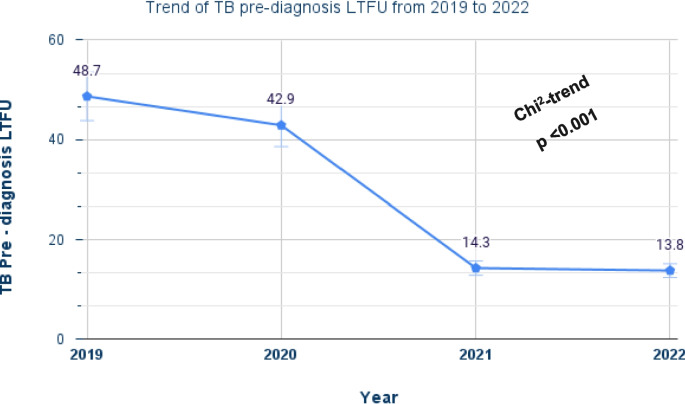
Background: Loss to follow-up (LTFU) of patients with presumed tuberculosis (TB) before completing the diagnostic process (pre-diagnosis LTFU) and before initiating treatment for those diagnosed (pre-treatment LTFU) is a challenge in the realization of the End TB Strategy. We assessed the proportion of pre-diagnosis and pre-treatment LTFU and associated factors among patients with presumed TB and those diagnosed in the selected health facilities.
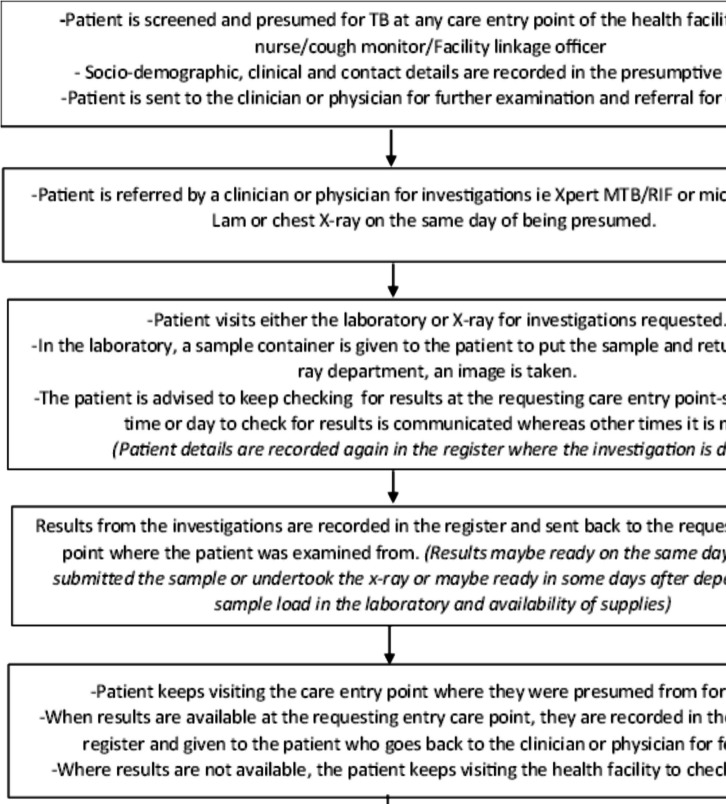
Methods: This was a retrospective cohort study involving a review of routinely collected data from presumptive, laboratory and TB treatment registers from January 2019 to December 2022. The study was conducted in three general hospitals and one lower-level health center IV in Central Uganda. We defined pre-diagnosis LTFU as failure to test for TB and obtain results within 30 days from the date of being presumed and pre-treatment LTFU as failure to initiate TB treatment within 14 days from the date of diagnosis. Modified Poisson regression was used to estimate prevalence ratios (PRs) and 95% confidence intervals (CIs) of factors associated with pre-diagnosis and pre-treatment LTFU.
Results: Of the 13,064 patients with presumed TB, 39.9% were aged 25 to 44 years, and 57.1% were females. Almost a third, 28.3% (3,699/13.064) experienced pre-diagnosis LTFU and 13.7% (163/1187) did not initiate treatment within 14 days from being diagnosed. Pre-diagnosis LTFU was more likely to occur among patients aged 0-14 years (adj PR 1.1, 95% CI: 1.06,1.24), females (adj.PR=1.06, 95% CI: 1.01, 1.12) and those with no record of place of residence (adj. PR=2.7, 95% CI: 2.54, 2.93). In addition, patients with no record of phone contact were more likely to be LTFU, (adj. PR=1.1, 95% CI: 1.05, 1.17). Pre-treatment LTFU was also more likely among patients with no record of place of residence (adj PR 7.1, 95% CI: 5.13,9.85) and those with no record of phone contact (adj PR 2.2, 95% CI: 1.63,2.86). Patients presumed from the HIV clinics were 40% less likely to experience pre-treatment LTFU compared to those in the outpatient departments (adj PR 0.6, 95% CI: 0.41,0.88).
Conclusion: High proportions of pre-diagnosis and pre-treatment LTFU were observed in this study. This calls for urgent interventions at these time points in the TB care cascade to be able to realise the End TB Strategy.
Keywords: Diagnosis loss to follow; Treatment loss to follow; Tuberculosis, loss to follow; Up, Uganda; Up, pre.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the Declaration of Helsinki [60]. Approval to conduct the study was obtained from the Research and Ethics Committee of Makerere University School of Public Health (#SPH-2023-427), and the study was registered with the Uganda National Council of Science and Technology (HS3000ES). The privacy and confidentiality of all the data obtained was ensured by limiting access of the data to only the study investigator and data manager. Since this was a review of records with no face-to-face interviews with patients, the need for informed consent was waived by the ethics committee. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Pre-treatment loss to follow-up and associated factors among drug-resistant tuberculosis patients diagnosed in Wakiso district, central Uganda.BMC Infect Dis. 2025 Jul 31;25(1):967. doi: 10.1186/s12879-025-11295-6. BMC Infect Dis. 2025. PMID: 40745635 Free PMC article.
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Undernutrition as a risk factor for tuberculosis disease.Cochrane Database Syst Rev. 2024 Jun 11;6(6):CD015890. doi: 10.1002/14651858.CD015890.pub2. Cochrane Database Syst Rev. 2024. PMID: 38860538 Free PMC article.
-
Delayed culture conversion predicts poor outcomes for isoniazid mono-resistant TB in Uganda: a retrospective cross-sectional study from 2017- 2022.BMC Infect Dis. 2025 Jul 1;25(1):821. doi: 10.1186/s12879-025-11218-5. BMC Infect Dis. 2025. PMID: 40597784 Free PMC article.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
Cited by
-
Pre-treatment loss to follow-up and associated factors among drug-resistant tuberculosis patients diagnosed in Wakiso district, central Uganda.BMC Infect Dis. 2025 Jul 31;25(1):967. doi: 10.1186/s12879-025-11295-6. BMC Infect Dis. 2025. PMID: 40745635 Free PMC article.
References
-
- WHO. Global tuberculosis report 2023. Geneva: World Health Organization; 2023.
-
- UN. The Sustainable Development Goals eSocialSciences; 2015.
-
- Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. WHO’s new end TB strategy. Lancet. 2015;385(9979):1799–801. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
