

Effects of two different dexamethasone dosing regimens on ventilator-free days and long-term mortality in COVID-19 patients with moderate-to-severe ARDS: the REMED randomized clinical trial
- PMID: 39710693
- PMCID: PMC11664838
- DOI: 10.1186/s40001-024-02215-6
Effects of two different dexamethasone dosing regimens on ventilator-free days and long-term mortality in COVID-19 patients with moderate-to-severe ARDS: the REMED randomized clinical trial
Abstract
Background: Dexamethasone 6 mg in patients with severe COVID-19 has been shown to decrease mortality and morbidity. The effects of higher doses of corticosteroid, that would further increase anti-inflammatory effects, are uncertain. The objective of our study was to assess the effect of 20 mg dexamethasone vs. 6 mg dexamethasone intravenously in patients with moderate-to-severe acute respiratory distress syndrome (ARDS) and COVID-19.
Methods: In a multicenter, open-label, randomized trial conducted in nine hospitals in the Czech Republic, we randomized adult patients with ARDS and COVID-19 requiring high-flow oxygen, noninvasive or invasive mechanical ventilation to receive either intravenous high-dose dexamethasone (20 mg/day on days 1-5, 10 mg/day on days 6-10) or standard-dose dexamethasone (6 mg/d, days 1-10). The primary outcome was 28-day ventilator-free days. The five secondary outcomes were 60-day mortality, C-reactive protein dynamics, 14-day WHO (World Health Organization) Clinical Progression Scale score, adverse events and 90-day Barthel index. The long-term outcomes were 180- and 360-day mortality and the Barthel index. The planned sample size was 300, with interim analysis after enrollment of 150 patients.
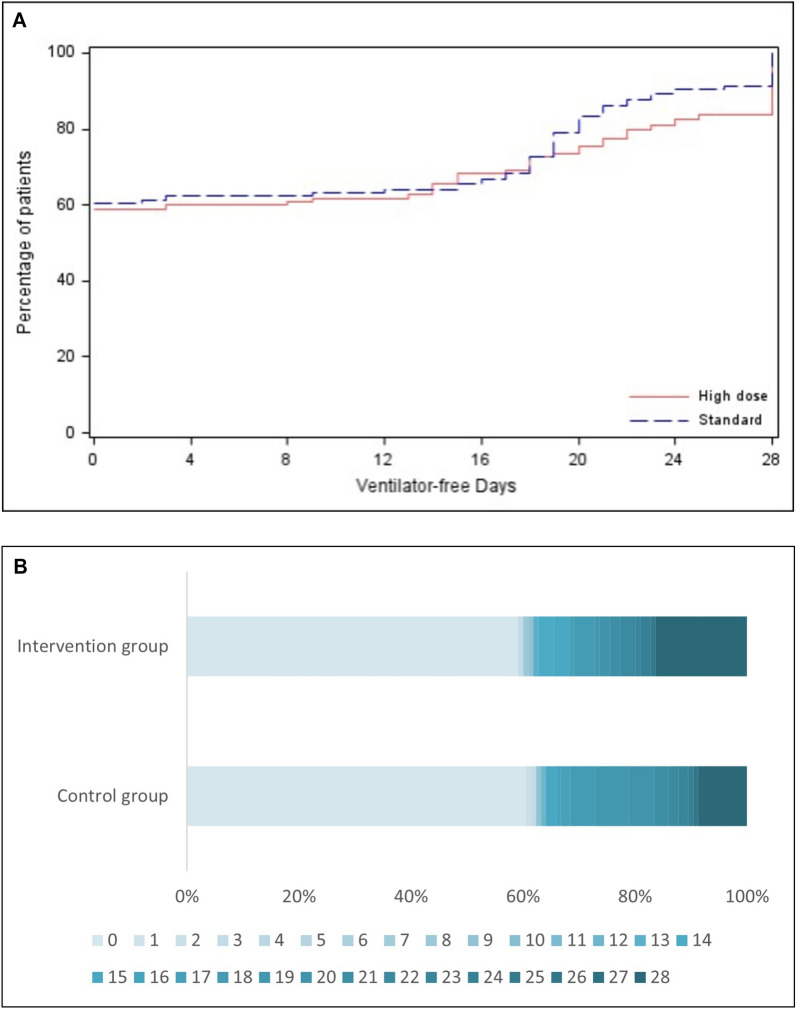
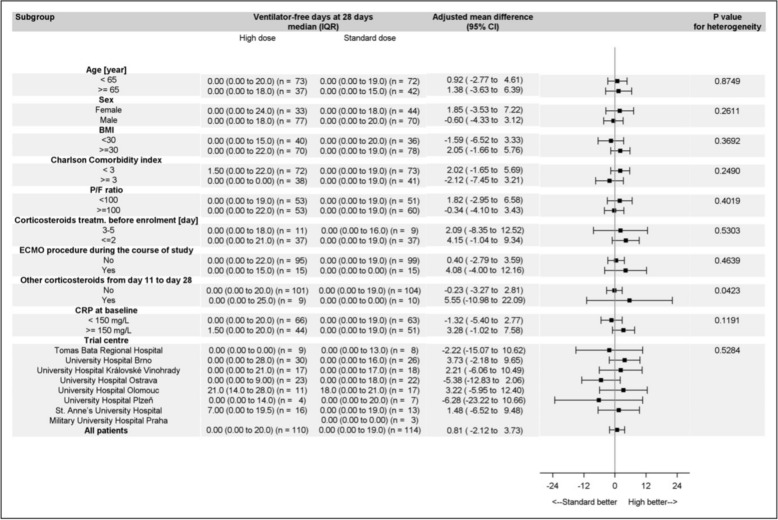
Results: The trial was stopped due to a lack of recruitment, and the follow-up was completed in February 2023. Among 234 randomized patients of 300 planned patients, the primary outcome was available for 224 patients (110 high-dose and 114 standard-dose dexamethasone; median [interquartile range (IQR)] age, 59.0 [48.5-66.0] years; 130 [58.0%] were receiving noninvasive or invasive mechanical ventilation at baseline). The mean number of 28-day ventilator-free days was 8.9 (± 11.5) days for high-dose dexamethasone and 8.0 (± 10.7) days for standard-dose dexamethasone, with an absolute difference of + 0.81 days (95% CI - 2.12-3.73 days). None of the prespecified secondary outcomes, including adverse events, differed between the groups.
Conclusions: Despite not reaching its prespecified enrollment, there was no signal to either benefit or harm high-dose dexamethasone over standard-dose dexamethasone in patients with COVID-19 and moderate-to-severe ARDS. Trial registration Trial registration: ClinicalTrials.gov Identifier: NCT04663555. Registered 10 December 2020, https://clinicaltrials.gov/study/NCT04663555?term=NCT04663555&rank=1 and EudraCT: 2020-005887-70.
Keywords: ARDS; COVID-19; Dexamethasone; Long-term outcomes; Randomized clinical trial; Ventilator-free days.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The trial protocol and consequent amendments were approved by the State Institute for Drug Control and Multicentre Ethics Committee of University Hospital Brno (Ref. No. 11/21MEK) and institutionally at each trial site. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Webb SA, Higgins AM, McArthur CJ. Glucocorticoid dose in COVID-19: lessons for clinical trials during a pandemic. JAMA. 2021;326:1801–2. - PubMed
-
- Villar J, Ferrando C, Martínez D, Ambrós A, Muñoz T, Soler JA, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8:267–76. - PubMed
-
- Bouadma L, Mekontso-Dessap A, Burdet C, Merdji H, Poissy J, Dupuis C, et al. High-dose dexamethasone and oxygen support strategies in intensive care unit patients with severe COVID-19 acute hypoxemic respiratory failure: the COVIDICUS randomized clinical trial. JAMA Intern Med. 2022;182:906–16. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
