

A retrospective, multicentric, nationwide analysis of the impact of splenectomy on survival of pancreatic cancer patients
- PMID: 39710775
- PMCID: PMC11663811
- DOI: 10.1007/s00423-024-03570-y
A retrospective, multicentric, nationwide analysis of the impact of splenectomy on survival of pancreatic cancer patients
Abstract
Objective: Splenectomy is regularly performed in total and distal pancreatectomy due to technical reasons, lymph node dissection and radicality of the operation. However, the spleen serves as an important organ for competent immune function, and its removal is associated with an increased incidence of cancer and a worse outcome in some cancer entities (Haematologica 99:392-398, 2014; Dis Colon Rectum 51:213-217, 2008; Dis Esophagus 21:334-339, 2008). The impact of splenectomy in pancreatic cancer is not fully resolved (J Am Coll Surg 188:516-521, 1999; J Surg Oncol 119:784-793, 2019).
Methods: We therefore compared the outcome of 193 pancreatic cancer patients who underwent total or distal pancreatectomy with (Sp) or without splenectomy (NoSp) between 2015 and 2021 using the StuDoQ|Pancreas registry of the German Society for General and Visceral Surgery. In addition, we integrated our data into the existing literature in a meta-analysis of studies on splenectomy in pancreatic cancer patients.
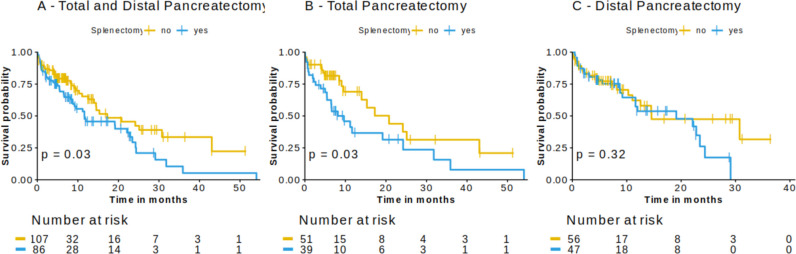
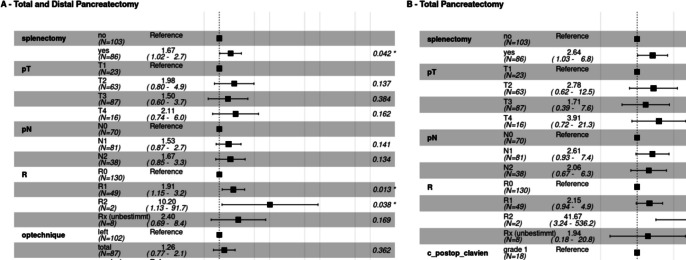
Results: There was no difference between the Sp and NoSp groups regarding histopathological parameters, number of examined or affected lymph nodes, residual tumor status, or postoperative morbidity and mortality. We observed a significantly prolonged survival in pancreatic cancer patients who underwent total pancreatectomy, when a spleen-preserving operation was performed (median survival: 9.6 vs. 17.3 months, p = 0.03). In this group, splenectomy was identified as an independent risk factor for shorter overall survival [HR (95%CI): 2.38 (1.03 - 6.8)]. In a meta-analysis of the existing literature in combination with our data, we confirmed splenectomy as a risk factor for a shorter overall survival in pancreatic cancer patients undergoing total pancreatectomy, distal pancreatectomy, or pancreatic head resection [HR (95%CI): 1.53 (1.11 - 1.95)].
Conclusion: Here, we report on a strong correlations between removal of the spleen and the survival of pancreatic cancer patients undergoing total pancreatectomy. This should encourage pancreatic surgeons to critically assess the role of splenectomy in total pancreatectomy and give rise to further investigations.
Keywords: Distal pancreatectomy; Pancreatic cancer; Splenectomy; Total pancreatectomy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
-
- Wakeman CJ et al (2008) The impact of splenectomy on outcome after resection for colorectal cancer: a multicenter, nested, paired cohort study. Dis Colon Rectum 51:213–217. 10.1007/s10350-007-9139-6 - PubMed
-
- Pultrum BB et al (2008) Impact of splenectomy on surgical outcome in patients with cancer of the distal esophagus and gastro-esophageal junction. Dis Esophagus 21:334–339. 10.1111/j.1442-2050.2007.00762.x - PubMed
-
- Schwarz RE, Harrison LE, Conlon KC, Klimstra DS, Brennan MF (1999) The impact of splenectomy on outcomes after resection of pancreatic adenocarcinoma. J Am Coll Surg 188:516–521. 10.1016/S1072-7515(99)00041-1 - PubMed
-
- Yang F et al (2019) Total pancreatectomy for pancreatic malignancy with preservation of the spleen. J Surg Oncol 119:784–793. 10.1002/jso.25377 - PubMed
-
- Warshaw AL (1988) Conservation of the spleen with distal pancreatectomy. Arch Surg (Chicago, Ill. : 1960) 123:550–553. 10.1001/archsurg.1988.01400290032004 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
