

Increased Early-Mortality in Children With Solid Tumors During the COVID-19 Pandemic in a Middle-Income Country
- PMID: 39711262
- PMCID: PMC11803909
- DOI: 10.1002/cam4.70483
Increased Early-Mortality in Children With Solid Tumors During the COVID-19 Pandemic in a Middle-Income Country
Abstract
Background: Measures to control COVID-19 transmission disrupted childhood cancer care. Data on the effects of the COVID-19 pandemic on childhood cancer mortality are lacking. This study describes the impact of the pandemic on childhood cancer early-mortality (≤ 24 months).
Methods: A multicenter prospective cohort was conducted in 10 Colombian cities. Children with newly diagnosed cancer registered in the Childhood Cancer Clinical Outcomes Surveillance System (VIGICANCER) were included. Our primary outcome was cumulative mortality at 3, 6, 12, and 24 months. The exposed cohort (EC = March 25, 2020-December 31, 2021) was compared with a historic cohort (HC = January 1, 2017-March 24, 2020). Covariates included sociodemographics, place of residence, health insurance type, and tumor classification.
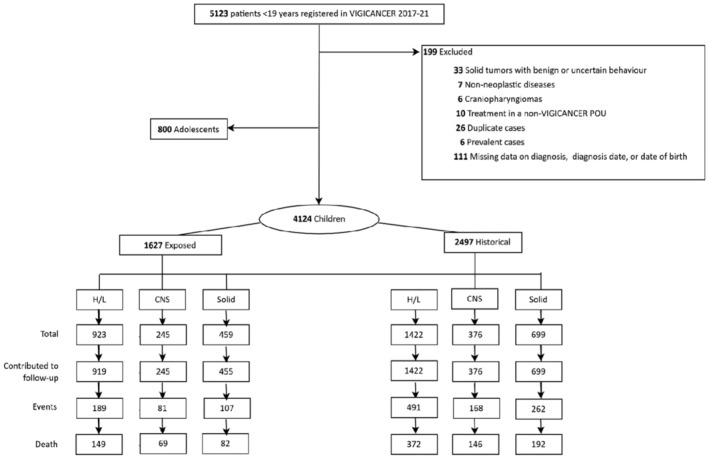
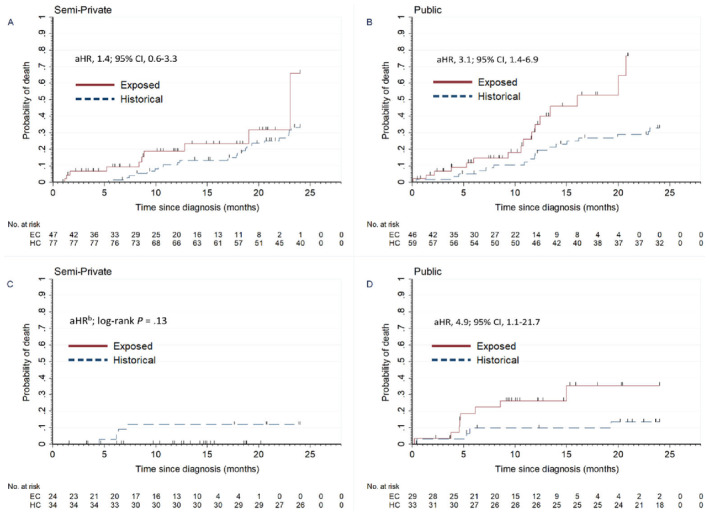
Results: The cohort included 4124 children, comprised of 1627 children in the EC and 2497 children in the HC. Hematolymphoid, central nervous system, and extracranial solid tumors represented 57%, 15%, and 28% of patients, respectively. Participants' median age was 6.7 years (IQR, 3.2-11.3), 54% were male, 7% were Afro-descendant, and 47% had public insurance. In the EC, the 6-month and 24-month mortality adjusted hazard ratio (aHR) in children with solid tumors was 1.7 (95% CI, 1.1-2.7) and 1.3 (95% CI, 1.0-1.7), respectively, and in children with bone tumors 4.0 (95% CI, 1.2-13.0) and 2.1 (95% CI, 1.2-3.6), respectively. These associations persisted after accounting for metastatic disease. Six-month mortality aHRs for retinoblastoma, bone tumors, and soft tissue sarcomas due to progressive disease were 4.3 (95% CI, 1.3-14.5), 4.0 (95% CI, 1.4-11.3), and 5.4 (95% CI, 2.2-13.5), respectively. In the EC, the adjusted odds ratio (aOR) for metastatic solid tumors vs. nonmetastatic was 1.4 (95% CI, 1.0-1.8) and in children with retinoblastoma and public insurance the 24-month mortality aHR was 4.9 (95% CI, 1.1-21.7).
Conclusions: We observed increased early-mortality for solid tumors, particularly bone tumors and retinoblastoma, likely attributed to more advanced-stage presentation and loss of treatment effectiveness due to healthcare disruptions. Early-mortality was higher in patients with public insurance, a vulnerable population that warrants attention.
Keywords: COVID‐19; bone neoplasms; epidemiological monitoring; hospital; mortality; neoplasms; oncology service; pediatrics; retinoblastoma.
© 2024 The Author(s). Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- World Health Organization , “The Impact of the COVID‐19 Pandemic on Noncommunicable Disease Resources and Services: Results of a Rapid Assessment” (2020).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
