

Update vulval dermatology - diagnostics and therapy
- PMID: 39711289
- PMCID: PMC11711937
- DOI: 10.1111/ddg.15541
Update vulval dermatology - diagnostics and therapy
Abstract
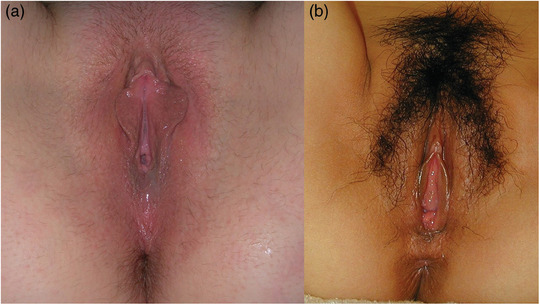
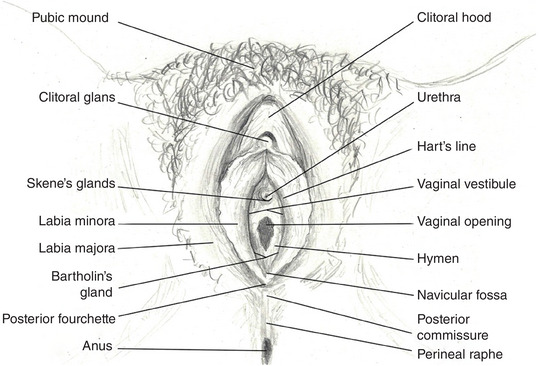
The vulva is a periorificial skin area and as such represents a transitional zone with unique functional and physiological characteristics. Knowledge of its anatomy is limited among both the general population and healthcare professionals, and unrealistic expectations of normal proportions are common. Ignorance of anatomical variations can cause unnecessary anxiety. In Germany, specialists in gynecology and obstetrics most commonly treat neoplastic vulvar dermatoses, while chronic inflammatory dermatoses commonly affecting the female genitalia (such as psoriasis, atopic dermatitis, hidradenitis suppurativa, and vitiligo) are typically treated by dermatologists. Both specialties treat infectious vulvar dermatoses and sexually transmitted infections. Certain dermatoses, such as lichen sclerosus, lichen planus, and lichen simplex chronicus, tend to affect the vulva preferentially; however, terminology can be confusing. Therefore, this article provides basic information on vulvar anatomy and physiology and summarizes recommendations for the diagnosis and management of the most common vulvar dermatoses, with a special focus on chronic inflammatory dermatoses, to provide a useful guide for all involved specialists in daily practice. Interdisciplinary collaboration and the establishment of dedicated consultation hours may help to improve the clinical care of vulvar dermatoses.
Keywords: Vulva; eczema; lichen planus; lichen sclerosus; lichen simplex chronicus; vagina.
© 2024 The Author(s). Journal der Deutschen Dermatologischen Gesellschaft published by John Wiley & Sons Ltd on behalf of Deutsche Dermatologische Gesellschaft.
Conflict of interest statement
The authors have received honoraria as speakers, advisory board members, travel reimbursements, or research support, or are involved in conducting clinical trials for the following companies: C.B.: L'Oréal, Novartis, Pfizer, UCB Pharma. L.W.: MSD, Roche, Eisai, Pfizer, Seagen, Novartis, GSK, AstraZeneca. D.N.: AbbVie, Almirall, AstraZeneca, Biogen, BMS, Boehringer‐Ingelheim, Eli Lilly, GlaxoSmithKline, Incyte, Kyowa Kirin, LaRoche/Cerave, L'Oréal, MSD, Novartis, Pfizer, Regeneron, Sanofi, UCB Pharma. The remaining authors declare no relevant conflicts of interest.
Figures



References
-
- Paarlberg KM, Weijenborg PTM. Request for operative reduction of the labia minora; a proposal for a practical guideline for gynecologists. J Psychosom Obstet Gynaecol. 2008;29:230‐234. - PubMed
-
- Lykkebo AW, Drue HC, Lam JUH, Guldberg R. The Size of Labia Minora and Perception of Genital Appearance: A Cross‐Sectional Study. J Low Genit Tract Dis. 2017;21:198‐203. - PubMed
-
- Pauls RN. Anatomy of the clitoris and the female sexual response. Clin Anat. 2015;28:376‐384. - PubMed
-
- Emmanuel M, Bokor BR. Tanner Stages. [Updated 2022 Dec 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470280/ [Last accessed June 1, 2024].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
